



2. School of Biomedicine, Far Eastern Federal University, Vladivostok, Russia;
3. NeuroVita Clinic of Restorative and Interventional Neurology and Therapy, Moscow, Russia;
4. Zhirmunskiy Institute of Sea Biology of the Russian Academy of Sciences, Vladivostok, Russia
Objectives: Significant advances in neurosciences will result from research focused on the non-contact treatment of the nervous tissue (NT). The objective of the article is to describe a novel non-contact method of restoration of damaged NT of the human brain and spinal cord that was termed multi-wave neuro-bioengineering.
Methods: The method includes a purposeful complex program of different therapeutic ionizing and non-ionizing electromagnetic radiation effects on the damaged NT, which is approved for clinical practice. Exposure of the human brain to a stepwise algorithmized combination of different ionizing and non-ionizing radiations and simultaneous application of various types of electromagnetic radiation at the specific site of restoration considerably reduce the adverse effects of all types of radiation on NT.
Results: The technology for non-contact restoration of the injured tissue of brain or spinal cord was appiled in 30 cases of neurological disorders using the stereotaxic system, structural resonance therapy, radiotherapy and focused ultrasound. The applied methods are approved for humans and theorem programmed combination opens new perspective for the treatment of brain and spinal cord disorders.
Conclusions: The approach provides quick restoration of the disordered function of damaged brain tissue and establishes a new paradigm of radio non-contact neurorestoration of the brain and spinal cord.
The standard therapies for brain disorders largely include pharmaceutical and rehabilitative/restorative treatments such as physiotherapy,exercise,massage, hyperbaric oxygenation,acupuncture,and phytotherapy. Contemporary therapy in the case of severe brain trauma and diseases produces similar outcomes in hospitals around the world: high mortality rate,or coma recovery resulting in a chronic vegetative state (e.g.,apallic syndrome or akinetic‐rigid syndrome) or the quick formation of an irreversible neurologic deficit[2].
1.1 Trends in the treatment of neurological injury and disease In the last two decades,multiple attempts have been made to restore the damaged brain through reconstructive neurosurgical treatment,although with a low success rate. The main methods for treatment remain the same: open reconstructive microsurgical interventions in the brain and the implantation of neuro‐engineered systems and devices. However,there is still no universal standard of a highly efficient protocol to restore human/mammalian brain and spinal cord that is approved by the regulatory bodies of the country. Furthermore,all currently existing methods to reconstruct the damaged brain and/or spinal cord are neurosurgical and microsurgical "improvisation" schemes in the plasty of the nervous tissue (NT)[3].A recent trend in the global clinical practice of brain restoration is a focus on reconstructing the morphological structure,relying on established technologies for interventional radiologic angioneurology and functional neurosurgery[4]. They are based on neuronavigation and minimally invasive neurosurgical interventions such as balloon angioplasty of brain vessels,stereotaxic radio waves and cry destruction of the NT,and implantation of stimulators,which are widely used in vascular neurosurgery,functional neurosurgery,neuroendoscopic neurosurgery,and radiosurgery. However,these surgical techniques did not allow for complete recovery from the original nervous and mental diseases,or for real morphological and functional restoration of the damaged brain and spinal cord in humans,irrespective of etiology or pathogenesis of the disorder[3].
An important breakthrough in therapeutic efficiency of neurological and spinal cord is expected within the next decade,as the natural result of the introduction of innovations from regenerative medicine (tissue engineering,cell transplantation,and cell therapy) to contemporary neurology and neurosurgery. In 2014, EU countries opened over 80 public institutions for regenerative medicine to treat neurological and psychiatric disorders,and over 300 similar centers will be established in the United States. To find the solution, the U.S. Department of Defense established the Wake Forest Institute of Regenerative Medicine and two research consortiums,involving 16 public universities each,and allocated over 300 million U.S. dollars. The functions of these institutions include the development of innovative technologies for regenerative medicine, including development of the neurotechnologies to restore the damaged brain. Recently,this field of medicine has become known as neurorestoratology[5].
The International Association of Neurorestoratology (IANR) considers invasive neurosurgical technologies of cell transplantation,tissue engineering,and bioen-gineering of the brain and spinal cord to be the main instruments and methods for neurorestoration[5]. The IANR actively supports the transplantation of stem cells for the reconstruction of the damaged brain/spinal cord,as well as the development of implantable bio‐constructions or artificial tissue (including NT) prosthesis for bioengineering and tissue engineering organs. The IANR promotes research that aims to search for and study optimal biomaterials, types of transplanted cells, culturing methods in bioreactors, types of scaffolds, and the mechanisms and patterns of neuroregeneration and neurorestoration along with opportunities to integrate a living biological construct into the brain or spinal cord in vivo.
Even with 30 years of scientifically based methodology and technology of cell transplantations,tissue engineering and neurorestoration,this has not led to the development of solid organs or tissues that structurally and functionally resemble the real thing. Existing artificial simulacra or organ equivalents (bladder,bone or trachea) poorly mimic the natural structure of mammalian organs,and require a significant functional update. Despite the fact that many of them have already been transplanted into humans, they are still far from ideal,and it will take a long time to make them more closely resemble their natural prototypes.
Currently,neural engineering is one of most rapidly developing trends in the biotechnological field, including bioengineering and tissue engineering of the brain and spinal cord. Wikipedia describes it as a discipline within biomedical engineering that uses engineering techniques to understand,repair,replace, enhance,or otherwise exploit the properties of neural systems. Neural engineers are uniquely qualified to solve design problems at the interface of living neural tissue and non‐living constructs. One review[6] gives a different definition: neural engineering is one of the tissue engineering fields and is based on neurophysiology, clinical neurology,and electrical engineering, and includes the elements of fields as diverse as robotics,cybernetics,computer engineering,materials science,and nanotechnologies. Neural engineering researchers aim to influence the recovery and augment of the functions of the human brain/spinal cord through various electronic and mechanic devices or computerized physical effects. Neural engineering is an inter‐disciplinary science that uses the methods and achievements of clinical and experimental neurology. It is a completely new discipline,in which the technical methods and laboratory equipment used for the research of the central and peripheral nervous systems are used to elucidate their function and control their reactions. The methodology of neural engineering presumes that in order to understand the essence of the neural processing,the science should learn how to register the activity of the nervous systems and to stimulate it. The current equipment already contained in neural laboratories makes this possible. The aim of the neural engineering is to understand the fundamental mechanisms underpinning cell signaling and synaptic transfer,which will allow for new technologies that copy these mechanisms with the help of artificial devices and interface with the nervous system at the cellular level[6].
The latest trend in the development of the innovative methods to treat the diseases of the brain and spinal cord is directed at the development of wireless, mobile,non‐contact,and preferably remote neural technologies. These innovative strategies combining contemporary neural sciences with clinical neurology and psychiatry were reflected in the documents of the Human Brain Project (ЕU) launched in 2012[7] and the Brain Initiative project started 2013 in the U.S.[8]. In December 2013,the Defense Advanced Research Projects Agency (DARPA) allocated multimillion grants for two new research projects within the Brain Initiative that aim at the development of new methodologies and technology of a wireless device that cures neurological disorders,as well as the equipment that will recover active memories. The first grant will support the Systems‐Based Neurotechnology for Emerging Therapies (SUBNETS),and,namely,the development of a new wireless device that would be able to cure such neurological disorders as posttraumatic stress disorder (PTSD),depression,or chronic pain[9]. The second grant will support the scientists who will succeed in Restoring Active Memory (RAM)[10]. They are planning to develop a wireless device,which will correct the damage to the brain and repair memory. This program includes a focus on the restoration of motor memories as well as more complex hierarchical memories. Although,these techniques are primarily meant for the injured U.S. army veterans,they can also be used to assist the civil population affected by similar neurological and psychiatric disorders.
At first glance,this non‐contact remote approach to treating neurologic diseases seems not only unrealistic, but also almost crazy and unrealizable. This reaction seems from the fact that most existing treatments of neurological disorders and injury a priori suppose a surgical restoration of the damaged tissue by manipulating the elements and/or components of NT. However,the mere fact that DARPA,a key generator of new scientific ideas and innovative technologies in all spheres,gives so much attention to treating this population,demonstrates the absence of technology to treat acute and chronic functional and organic pathologies of the brain and spinal cord. Their technical specification in the development of these devices sets a very high standard to utilize highly technological methods in treating insults to the brain and spinal cord,which is hard to achieve without specific contemporary equipment,methods,and technology.
Our experience with neurosurgical and regenerative technologies in the restoration of the brain imbues us with the sense that DARPA’s initiative to develop noncontact technology for the remote restoration of the brain tissue is not as unrealizable and crazy,as it may first seem. We suppose that the goal will be a nonsurgical, but complex highly technological solution, based on a combination of technologies that allow for remote multi‐level (with different wavelengths and frequencies) electromagnetic effects on NT. We think that the available and clinically approved methods of electromagnetic effects on NT of the brain and spinal cord can realize DARPA’s ideas. As such,we has attempted to work out a practical example of using this technology in neurological patients and the demo version of the device to implement it.
1.2 The purpose of this article The goal of the article is to present the principles underpinning the novel neural technology for noncontact remote reconstruction to damaged human NT and a stereotaxic helmet through which to conduct the therapy through emitting different types of electromagnetic waves (EMWs).In summary,we think that the proposed neurotechnology to restore the injured brain can be considered a neuroengineering technology,and that the use of medical equipment for stereotaxic ionizing effect (stereotaxic radiotherapy and radiosurgery) and electromagnetic non‐ionizing wave effects (structural‐resonance therapy, focused ultrasonic therapy) inherent in the technology allows us to discuss the remote reconstructive focused multi‐level radio‐bioengineering effects on the NT of the brain or the radio‐bioengineering method to restore the injured NT of the human brain and spinal cord. Thus,we propose an alternative to contemporary neurosurgery, namely,the neurotechnology consisting of a remote stereotaxic program of multi‐wave neuroengineering that can be used to treat a wide range of nervous and mental diseases in humans and other mammals.
2 Materials and methods The technology of remote multi‐wave radio-neuroengineering was developed with 30 neurological cases and was meant for the remote reconstruction of the damaged NT of the human and mammalian brain and spinal cord in the case of acute,sub‐acute and chronic neurological and residual neurological and mental diseases of the brain. Depending on the dominant pathological process in damage to the brain or spinal cord (degenerative atrophic process or reproductive proliferative process),the standard and approved modes for treating NT damage were used according to the technical recommendations and characteristics specified by the manufactures of the medical equipment. Visual computer diagnostics of physiological NT damage (using magnetic resonance imaging,positron emission tomography/computed tomography,cerebral mapping,electroencephalography, magnetoencephalography,electroneuromyography, etc.) to detect the sites of brain/spinal cord reconstruction was done with certified medical equipment. The structural‐resonant effects on the brain and spinal cord were achieved using certified equipment for electromagnetic therapy,which is approved for clinical practice in the Russian Federation: a contact electrostimulation array for structural resonance therapy REKELSI NPKU.941514.001 with automatic and manual modes for light and sound stimulation, designed to correct structural and functional conditions in tissues and organs when resonating with regulatory systems of microcirculation,nerve conductance and cell structures. The restorative effect of focused ultrasound (FUS) on the brain/spinal cord was achieved in two ways: (1) Use of the computerized equipment for MR‐guided FUS ablation where the ultrasound is focused with electronic phase‐shifting occurring due to the combination of spherical and linear spatialtemporal interrelationships between the impulses received by the transducers,thus,allowing the ultrasonic field to focus at prescribed distance and spread at specific azimuth angle. (2) Use of a stereotaxic system with holders for ultrasound transmitters, allowing for the alignment of separate impulses received from the transmitters of the ultrasound apparatus (the apparatus for ultrasound therapy AST‐1.01F) thus resolving the issue of azimuth navigation and directing ultrasonic waves to specific sites in the brain/spinal cord. The stereotaxic radiosurgery Cyber Knife system was used to maintain the effect of ionizing radiation (IR) on the human brain/spinal cord for remote multi‐wave radio neuroengineering. All equipment has been approved for clinical application in the Russian Federation. 3 Experimental 3.1 The methodological prototype for remote multiwave radio‐neuroengineering It is obvious,that any newly developed therapeutic method for treating neurological and psychological disorders must involve new advances in the techniques utilized for diagnosis and therapy in neurology, psychiatry,neurosurgery,neuro‐oncology,radiosurgery, and regenerative medicine. However,the issue for non‐surgical reconstruction of the NT of the brain can be solved only in an unconventional,asymmetric, and non‐linear way,that is,by a radical departure from the basic physical principles underpinning the treatment,methodological approaches,and available technology for brain reconstruction. The issue of the remote restorative effects on the NT of the brain can be solved with a fundamentally new biotechnological method. We think the solution can be found in the distant combined multi‐wave program electromagnetic effects on the injured NT of the human brain and spinal cord.The development of radio‐neuroengineering technology resulted from the scientific,methodological, and practical developments achieved by our team in medical radiology,physiotherapy of nervous disorders, cell biology,tissue engineering,and bioengineering of the brain in animal models and clinical trials of these methods in humans. The development of the described method to treat nervous and mental disorders is associated with our 25 years of experience in the development and clinical use of regenerative medicine approaches in the treatment of combat injuries and transplantation of fetally derived neural cells (550 cases)[11],and in the transplantation of autologous hematopoietic stem cells (HSCs) and progenitor cells (PCs) that were mobilized into the peripheral blood of patients with physiological disorders of the central nervous system (CNS) (5230 cases)[12]. For over 12 years we used these novel techniques of tissue engineering in the brain and spinal cord in animal and human trials,involving biomaterial of fetal stem cells and biopolymer matrixes (52 cases of the spinal cord injury)[13]. We worked out,patented and successfully implanted an autologous cell‐biopolymer neuroendoprosthetic system in 52 cases of severe spinal cord injury (SCI),which was based on a Russian approved biodegradable polymer matrix "SpheroGel©"[14]. The development of this technique is published in 125 articles and 5 specialized monographs,as well as patented in several Russian patents and filed international patent applications.
We have critically evaluated our longstanding surgical experience in cell transplantation and tissue engineering to reconstruct the injured brain and spinal cord in animals and humans,weighing the pros and cons of the current open neurosurgical operations and interventional radio surgical technologies of tissue engineering for neural restoration of the NT. We also sum up the complications and negative outcomes and make a rather controversial conclusion. It appeared that the best results were observed in cases where cell therapy and tissue engineering were applied to the brain or spinal cord and when the extent of direct or indirect neurosurgical or transfusion cell intervention into the brain or spinal cord was minimal. The less surgery‐associated damage there was to the tissue, the better were the resulting,long‐term benefits of the therapy. The optimal results in the treatment of neurological and psychopathological disorders of the brain and spinal cord were obtained from regenerative approaches with a simple intrathecal administration of the HSCs preparation (55.4% of positive results) into the subarachnoid space in SCI cases,and not from highly technological neurosurgeries involving tissue engineering[12].
The basis of this innovative radio‐neuroengineering technology is the patented,minimally invasive technology to bioengineer of the brain and spinal cord[13]. During the 1990s and 2,000s,we worked on an approach to reconstruct the human and mammalian brain and spinal cord,using minimally invasive surgical techniques of functional stereotaxic neurosurgery, radiosurgery,and neuro‐endoscopy,and implemented them in the clinic. We elaborated this bioengineering methodology and approach to restore NT of the damaged brain or spinal cord through an algorithmized stepwise surgical application of minimally invasive technologies,radio opaque contrast instruments and materials (implantable balloons,stents,perfusors, conductors,etc.),radiosurgery,functional stereotaxic neurosurgery and cell transplantations,as well as implantation of neurostimulators,neurosystems and electronic devices. The basis underlying this program of stepwise reconstruction of the damaged brain or spinal cord appeared quite viable and knowledgebased. The technology of neural reconstruction involved a series of consecutive steps (algorithm) of the minimally invasive bioengineering: (1) the design stage, (2) the remodeling of the vascular bed stage, (3) the cell transplantation stage, (4) the dynamic integration of somatic and vegetative components stage, and (5), the rehabilitation stage (Figure 1). For a better understanding of the content of each methodological stage,we would like to describe each stage in detail and discuss its advantages and disadvantages.

|
| Figure 1 A scheme of bioengineering method of repair of the disordered function of the brain in the prototype technology. |
At the beginning,the design stage in the locus of the brain/spinal cord lesion is detected by visual analysis of the CT and MRI data. The vascular modeling stage involves the construction of extra micro‐vascular collaterals at the site of injury. Remodeling of vascular bed was done with minimally invasive radiosurgery, involving a puncture of the femoral vein,placement of the introducer,intra‐arterial radiosurgical placement of the perfusion catheter as close as possible to the site of the lesion in the projected reconstruction of the vascular pool,and finally,regional perfusion of vasoactive agents such as vazaprostan,papaverinum, and drotaverin for 24‐48 hours. Thus,the total surface of capillary network at the site of restoration was typically enlarged 5‐6 times,and,occasionally up to 10 times. In the cell transplantation stage,the missing cellular components at the lesion site were replaced with a functional stereotaxic neurosurgical or open surgical transplantation of neural stem cells into the brain parenchyma. Restoration of the cellular NT components was achieved through direct cell transplantation,which promoted the restoration of quantitative aspects of the cellular composition at the site of the lesion and restoration of synaptogenesis, i.e.,the damaged synaptic connections between the neurons. Specifically,this stage involved the transplantation of cells cultured from fetal,allogeneic,or autologous neural stem cells or hematopoietic stem cells,using neurosurgical equipment (stereotaxic equipment and the system of neuro‐navigation) or, using intraventricular and intrathecal transfusions of the cells[13]. The stage of treatment of the autonomic nervous system in the prototype technology implied mini‐surgeries or interventional manipulations. For this,sympathectomy was performed on the side with the injury,with procaine application to the sympathetic ganglia or transplantation of neural cells into the sympathetic ganglia[13]. To restore the vegetative or cellular‐tissue relationship at the lesion site in the dynamic integration stage of somatic and vegetative components,electrodes with standard electric stimulators were implanted into the projection of the zone where the tissue of the brain/spinal cord was being reconstructed either subdurally,intracerebrally,or, alternatively,into the Trancranial magneto stimulation of the brain/spinal cord was performed. This stage of rehabilitation of the NT was performed according to accepted protocols for the physical treatment in neurological cases: physical rehabilitation on the training equipment,physiotherapy,exercise,massage, etc.).
The patentability of this prototype technology was allowed through the novel methodology we developed and the multi‐stage treatment algorithm of minimally invasive bioengineering,which ensured the complexity and quality of the restoration of the morphological structure for the damaged NT. The effectiveness of this patented multistage minimally invasive surgical application of biotechnology in the reconstruction of the brain/spinal cord was clinically confirmed in the central interdisciplinary naval clinical hospital over a span of several years (1996-2000). The use of this approach has allowed for a reduction in the mortality rate by 15% in combat‐related brain trauma,and a reduction in the disability rate by 35% in the wounded[13].
3.2 The limitations of the clinical use of the prototype technology Despite multiple benefits from this minimally invasive bioengineering technique we used in the clinical practice of military medicine,a key unsolved issue in the procedure led to severe iatrogenic surgical complications (subarachnoid and subdural hemorrhages in the NT of the brain/spinal cord,ischemic strokes, purulent‐septic meningitis,meningoencephalitis,comas, septic complications,etc.),that developed throughout all stages of this technique. Given that there is no surgery without complications,and at that time (1996-2000) we had to work with a severely injured patient cohort,these complications were treated as inevitable even with our interventional radiosurgical and functional neurosurgical techniques to treat combat injuries.Without any doubt,over the last decade of the 20th century this method leading to the repair of neural tissue in patients with severe trauma was a breakthrough for reconstructive neurosurgery in the treatment of combat injuries to the brain,but these large numbers of complications became a central reason to restrict its application from civilian health care. However,this was not the only limitation that restricted this bioengineering protocol from mainstream introduction into civil health care.
Another serious disadvantage of this technology is the minimally invasive bioengineering of the brain is considered for only large morphological lesions of the brain/spinal cord that were visually identified in MRI and CT imaging,while minor injuries of the NT, neurophysiologic,metabolic and functional aspects of the lesion were not taken into account. Minimally invasive radio‐ and endo‐videosurgery technologies did not allow for the treatment of minor or multiple lesions in the brain.
A third significant drawback of this minimally invasive bioengineering technology is its high cost. The cost of contemporary radiosurgical and neuronavigational equipment and specialized expendables for the radiosurgical intervention and other consecutive steps of the brain bioengineering keeps expanding in an arithmetic progression,since we use foreign miniimplants and implantation materials. This year alone the costs of the expendables for the radiosurgical manipulations,neuroendoscopic interventions and functional neurosurgery increased by 30%-45%. The implantable electronic neurostimulators are also quite expensive,for example,the price for Medtronic neurostimulator varies from $18,000 to $25,000. The high costs of these expendables result in a high cost for surgical work utilizing these materials. The challenge to reduce these primary expenses for the treatment of brain/spinal cord injuries induced the search for a new import‐substituting alternative and less expensive methods of treatment.
We also have noticed a lack of effectiveness in contemporary technologies for tissue engineering and bioengineering of the brain,which is complicated by the fact that existing methods for the transfusion of allogeneic cells,autologous HSCs and hematopoietic progenitors are generally uncontrollable. The major component of the expensive cell biomaterial that is administered intrathecally and is able to provide regenerative,neurotrophic,stimulating,proliferative and regulatory effect in the site of injury,deposits itself on the meninges of the brain or is withdrawn from systemic blood circulation and bone marrow or from different organs,while the other part is lysed by cerebrospinal fluid (CSF).
If the cells are administered intra‐arterially or intravenously,they are not capable of reaching the areas of reconstruction due to exclusion by the protective blood brain barrier (BBB),which is normally impermeable to regulatory mononuclear cellular elements of the blood,stem cells (SCs) progenitor cells (PCs),as well as the majority of neurophilic drugs. Thus,the BBB cannot be passed by HSCs,mesenchymal stromal cells or other biologically active agents. These therapeutic substances are physically unable to enter the site where the brain/spinal cord reconstruction is occurring in sufficient amounts. Conventionally,most components of the cell systems we developed build up in different organs and tissues or go back to the niches of the bone marrow.
There is unquestionable scientific evidence that a maximal concentration of the cell preparation must be achieved in the site of reconstruction of the brain/ spinal cord,which will be the cornerstone for tissue restoration and regulation of its functional properties and characteristics[14]. To date,the tissue engineering surgery has accomplished this,holding the cell systems within the heterogeneous scaffolds of biopolymers that are implanted into the lesion site. The efforts of the specialists to provide a maximal concentration of SCs to the reconstruction site are the key element underpinning the whole mechanism for the replacement of the damaged cell systems.
In addition we searched for biochemical (liposomes, biopolymer capsules around the cells,nanostructures, etc.) and/or immunochemical (immunoliposomes, vectors attached to the cells and antigenes or antibodies molecules) systems for targeted vector delivery of the molecular components of a pharmaceutical or cellular preparation to the injury site or the restoration of the tissue of the brain or spinal cord. However,these approaches are not physiological; on the contrary,they are traumatic to the internal structure and alter homeostasis of the tissue they are meant to repair. Such "rubbish",as the fragments of liposomes,elements of antibodies or microparticles of the biopolymer and metal beads,left in the tissues after administration,is impossible to remove from the intercellular structure of the human organs and tissues.
Other important challenges and clinical paradoxes for regenerative medicine in general,and neurorestoratology of the brain and spinal cord,in particular,are the issue of the "structure and function" for the reconstructed NT. Apparently,it is impossible to develop a universal construct a priori,which would exactly replicate the delicate balance of the structural and biological properties and the natural matrixes and the cellular systems of the NT. Many tissues,when studied at an extreme magnification,exhibit occasional organization.
Nature functions in such a way that everything has its systemic and structured organization. This is the reason why the development of a new biological structure in the engineered tissue system allows hope for the restoration or replacement of the lost function of the organ or tissue. This idea can be applied to any methodology for human brain restoration.
Our longstanding experience with neurosurgical reconstruction of the injured brain shows that complete neurosurgical restoration of the anatomical completeness of the NT in the injury site and even moderate neurophysiological restoration of electrical conductance through the reconstructed site of the brain/spinal cord,does not entail a complete restoration of the function in most cases. At the same time,in some cases with minimal treatment,such as treatments involving two or three administrations of the cellular preparation to the old morphologically rough scarcicatricle or polycystic defects of NT of the brain or spinal cord,triggers the lost function of walking,restoration of sensation and,most frequently,copulative function,without the restoration of anatomical integrity. The reason for such unusual clinical phenomenon lies in the plasticity and the development of the new synaptic contacts established between the axons of damaged neurons[15]. Scientific evidence of this type of synaptogenesis is one of the most well known and convincingly proven biological phenomena that explains one of the fundamental mechanisms underlying the effects of administering cellular preparations to the brain/spinal cord[14]. Therefore,it is quite possible to restore electrical conductance in the damaged area of the brain by promoting synaptogenesis; and it can be achieved through the secretion of neurotrophic factors from the cellular preparation on local synaptogenesis,which is followed by the physiological restoration electric impulse conductance between neurons. However,this does not solve the problem even though a maximally intensive restoration of the quantitative values of electric conductance in the nerves is achieved,the neural regeneration of the NT cannot guarantee a full restoration of the quality of the information transfer in the NT,which does not provide for the restoration of lost functions.
Another important yet unsolved challenge of neurorestoratology,tissue engineering and minimally invasive bioengineering of chronic injuries of the brain and spinal cord in humans,is the compensatory development of rather stable cicatricial and/or cystic transformations of the tissue and an insufficient cellular‐vascular structure of the NT at the lesion site[16]. The newly formed pathological vascular connections in injured brain/spinal cord region are very stable due to gliosis. Although,these vascular connections do not provide an improvement to functioning, they are quite stable and resistant to any external influences from the cellular microenvironment which are not eliminated by common regulatory signals of the transplanted intact SCs and PCs.
The described flaws of this minimally invasive bioengineering technique in the brain can be overcome with a new technological aspect of scientific progress in medicine. The tasks of neurorestoration that we solved with the help of these minimally invasive surgical methods can be realized in a remote way today,without a direct contact of the surgeons’ hands and with tools within the NT of the human brain. The methods and multilevel,non‐contact electromagnetic wave effects on the brain and spinal cord for the purposeful morph functional reconstruction and neurorestoration can be an alternative to the minimally invasive radiosurgery,functional neurosurgery,and endovideosurgery approaches. Consequently,the systemization of these technologies and methods for remote electromagnetic wave effects on the NT of the brain became the central reason for our attempt to realize similar effects resulting from bioengineering plasty without the use of any invasive or surgical technologies and instruments.
3.3 The novelty of the developed technology The novelty of this technology lies in the innovative method developed for the reconstruction of the brain/ spinal cord NT through remote radio manipulations within the NT structure and the combination of remote non‐invasive and non‐surgical control of these molecular processes,cell systems and molecular‐cellular mechanisms in the appropriate site of the injured NT. In our approach,the radio‐neuroengineering technique is based on molecular‐wave,non‐contact mediated correction of the morphofunctional condition of the NT within the brain/spinal cord and manipulations of the intracellular structure in the injured NT through different types of radio‐therapeutic radiation and management of the affective properties (mobilization, homing,path tropism,cell adhesion,by‐stander effect) of autologous cell systems from the progenitors of hemopoiesis. The effects of ionizing (Χ-ray) and nonionizing (electromagnetic‐wave) regulatory (focused ultrasound and structural resonant) molecularcellular stereotaxic application to the lesions of the brain/spinal cord NT are purposeful for non‐contact engineering reconstruction of the NT. The proposed therapeutic methodology excludes any type of neurosurgical intervention (open,functional,radiosurgical and endoscopic) or direct invasive instrumental contact of the manipulator with the reconstruction target.We decided to preserve the methodology and algorithm from the stages of the brain reconstruction of the previously discussed non‐contact remote technology of neurorestoration in an identical fashion to the algorithm of minimally invasive surgical restoration of the brain/spinal cord. The stages of NT restoration were realized through consecutive use and exploitation of well‐known scientific evidence and neurobiological phenomena of the brain/spinal cord NT in response to different types of electromagnetic stimulation. Apparently,all methods of electromagnetic stimulation on the brain are known and described in the literature: the equipment for electromagnetic stimulation is standardized and certified for the treatment of psycho neurologic cases,and we have systemized a well described phenomena and reactions of the NT to different types of electromagnetic effects and established a new algorithm for their application to the innovative technology for non‐contact remote reconstruction of the damaged brain/spinal cord.
3.4 The neurobiological phenomena observed in the human brain/spinal cord when applying different types of electromagnetic radiation (EMR) We studied and summed up known evidence about the neurobiological effects of EMR in the NT of the brain/spinal cord. Table 1 represents the scale of EMR used in medicine,and is listed based on the wavelength and EMW range. As seen from this table, almost the existing EMW range can be used for NT restoration. However,for remote neurorestoration we used only three main wavelengths of focused EMWs: (1) Ionizing radiation in the ray range (λ = 10-0.000 nm).(2) Focused ultrasound (FUS) λ = 1-10 cm of super high frequency (SHF) of EMWs. (3) Structural resonant effect (SRE) of super‐low frequency (SLF) EMWs (λ = 1-10 mm).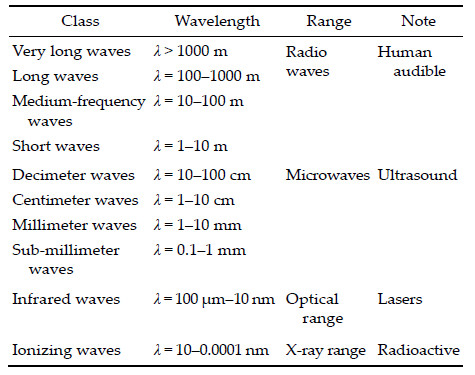
Obviously,all types of EMWs exhibit the features necessary for the reconstruction of the brain/spinal cord. We will discuss only the main neurobiological effects that occur in the NT from the application of various EMWs. The effects of the interaction of EMWs with different biological objects are subdivided into the effects from ionizing radiation (IR) and non‐ionizing radiation (nonIR)[17]. Usually,the IR occurs from the electromagnetic oscillations (optic,Χ-ray and gamma), the energy quantum of which is so strong that it can disrupt intermolecular bonds or ionize an atom. Electromagnetic oscillations of longer wavelength with lower quantum energy are known as non‐IR.
The interaction of EMWs with the biological subject is determined by the specific characteristics of the radiation (frequency,wavelength,propagation velocity, coherence of oscillations and wave polarization) and by the properties that a biological subject where the EMW spreads (dielectric permittivity and electric conductance),as well as the specific variables of their interaction (length of EMW in the tissue,penetration depth and reflection coefficient at the tissue‐air border). Hence,the reduction in the amplitude when EMW penetrates the tissue can be characterized by the penetration depth O: the distance,at which the amplitude of oscillations are reduced e ~ 2.72 times. This results in an increase in the permeability of the tissue for high frequencies. For example,Χ-rays and gamma rays penetrate soft tissue un‐attenuated. The typical example of the effect of radiation on the organism is hyperthermia when the useful effect is achieved when the energy of EMR transfers to heat. However,there can be an effect accompanied by a slight temperature rise ( < 0.1 degree),but this does not appear to alter the useful effects. In such cases,we speak about the controlling or information effects of EMR at a low or non‐thermal intensity. The research showed that this feature is characteristic for EMR of millimeter waves with a low‐density power flux that makes fractions or a single unit of milliwatt per 1 cm2 reaching the radiated surface (wavelength of radiation in free space from 1 to 10 mm).
To date we have evidence that the radiation induces the molecular and cellular basis for the cerebral effects caused by low doses of IR: disordered neurogenesis in adult hippocampus,changes in gene expression, neuro‐inflammatory reactions,altered neurosignaling, apoptosis,secondary cell damage,and other effects. These disorders along with other well‐known vascularglial associations seem to account for the pathogenesis of radiation damage in the brain[18]. On the other hand, it has been proved that low doses of IR can be used to stimulate the regeneration of tissue[19] accompanied by short‐term changes in the condition and permeability of the BBB[20]. The minimally safe regimen of ionizing electromagnetic radiation on the human brain is 1Gy,and tolerable fraction dose is 0.1 Gy. We consider this regimen to be practical and reasonable and will be our therapeutic goals.
Still,it should be noted that a range of important issues and challenges limit broad clinical adoption of different methods for the application of IR EMWs. Currently,there are two essential challenges in radiobiology and radioprotection that limit their broad application. The first is the influence of low doses of IR on human health in general and the potential IR‐induced NT damage in particular. The second challenge involves an approximately hundred‐yearold discussion about radio sensitivity/vulnerability of the human brain. The combination of these unsolved issues,specifically whether low doses of ionizing radiation damage the brain,is a very controversial problem. According to the law established by Bergonie and Tribondeauin 1906,"the radiosensitivity of a tissue is directly proportional to the reproductive activity and inversely proportional to the degree of differentiation." Accordingly,mature NT is viewed as an exclusive example of "a closed static population" and this cellular population is considered to be the most radio resistant due to its stable post‐mitotic state. Nonetheless,more and more accounts about radio sensitivity of the CNS are published each year[21]. Meanwhile,the benefits of low doses of radiation for humans have been recently reported again,which are considered to be a "radiation‐adaptive response"[22]. Moreover,it is considered that the "vascular‐glial association" provides the cerebral basis for postradiation damage of the brain,while the neurons are considered to stay outside the pathogenesis for radiation damage. Accordingly,the white matter of the brain must be more vulnerable to radio waves than grey matter. Recent advances in the understanding of radiation damage to CNS tissue revise these firmly established concepts. By now,it has become clear that the CNS is the main dose limiting system for the application of clinical radiotherapy[21],as the CNS is very radiosensitive.
Hypersensitivity of the nervous system to EMR of non‐ionizing radiation is well known. This can be confirmed by the neuropsychiatric disorders that occur in people who have long‐term exposure to radiation sources. The SRE on the brain and spinal cord of patients and formation of the resonance to the EMR frequencies deserves a special discussion. The idea of biological resonance multiplies the effect of EMWs, when the affecting frequency coincides with the frequency of the subject. It is important not to confuse the SRE response with other popular "bioresonances", Voll resonances,neuromodulations,resonance neurostimulations as well as others what make electromagnetic structural resonant therapy (SRT) unique is the correct physiological effects of applying an alternating electric current of a specified type,amplitude, and frequency that are chosen depending on the frequencies of the spontaneous bio‐potential activity in the patient’s organs and tissues. Thus,the conditions necessary to restore genetically conditioned rhythms of human people according to the law of resonance are established. Hence,the therapeutic opportunities for this technology are very broad and the absence of stimulation elements and heating reduce the risk of side effects and complications.
It has been shown that external (electric and electromagnetic) signals of EMR within the frequency of specific biological rhythms represented as SRE, affect different levels (cellular,organ, and tissular) and their regulatory pathways (nervous,humoral, and energetic). The method of structural‐resonance electromagnetic therapy (SREMT) was proposed to produce selective remote effects on different levels of the organism. The methods for electric current exposure were developed by the research team of Central Medical Sanitary Unit No. 165 of the Federal Medical Biological Agency of Russia[23],laboratory of clinical pharmacology of Sechenov Moscow Medical Academy and the Department of Theoretical Issues of Non‐Pharmaceutical Therapy of the Research Institute of Traditional Methods of Treatment and Diagnostics. For general, systemic,low‐intensity electromagnetic fields exposure, a special device known as REMATERP is used. For local exposure a device known as a KELSI‐01‐MSK and RADOMYS‐MSK is used. The frequency ranged from 0.026 Hz to 360 000 Hz to affect all levels of the structural organization: cellular,tissular and organ. The therapeutic effects of low frequency magnetic therapy and specifically the pain relieving,antiinflammatory, regenerative,and immune‐correcting responses are inherent to the electromagnetic type of SRT. Also,SRT is one of the non‐surgical methods used to treat microcirculation disorders at the site of brain reconstruction and can normalize and regulate the cellular‐vascular micro‐capillary network at the injury site[23].
When the molecules of nerve cells are exposed to non‐IR,the energy is spent on the transition of molecules from one energy state to another,which correlates with the optical range. If we look at relatively large structures,the rotational or vibrational transitions correspond to the microwave band. If the radiation frequency coincides with the rotational frequency of polar molecules,a resonance transition in the energy of the molecular radiation is possible. In such an interaction,the structure of this molecule does not change,but its rotational energy increases. For the efficiency of this energy interchange,it is important that the process is long‐term,and the energy dissipation is minimal. For the molecules of water,the resonant transition of energy is accompanied by its rapid dissipation caused by collisions of the molecules. That is why it is impossible to visually observe the resonant character of an interaction experimentally[23].
Interaction of electromagnetic non‐IR with the biological medium at different organization levels is well studied: from separate atoms and molecules to the simplest structures,such as the membranes or cellular infrastructures. The magnetic component to the EMR effects can be associated with paramagnetic orientation of the affected molecules,as well as a change in the trajectory of a moving charged particle (Lorenz effect). The mechanism for the electric component effects is associated with the oscillatory movement of free charges (electrons and ions). This electric component can change the orientation of the molecules that initially have dipolar moments. As the medium has an inherent electric resistance and viscosity,energy is lost in it. Such processes may depend on the radiation frequency,but will hardly be very critical to it,as it is characteristic for biological experiments[24].
The effect of SRE on the injured brains of patients is also studied well. A team of Russian researchers[23] analyzed the known bio‐effective frequencies,experimentally detected and calculated (according to the method of Chirkova EN) resonant frequencies for different organs and tissues of the human body,which allowed for the development of an integral system (a kind of periodic system of structural‐resonance frequencies for different organs and tissues) that was used as the basis for the specialized equipment used to apply SREMT in humans. According to the researchers, the periodic system of structural resonant frequencies of human organs and tissues results from the matrix of the management of all physiologic processes and life activities. The physical processes that carry information electromagnetic signals of appropriate frequency,type and other characteristic,achieve the management of all processes. Having received such a signal,the subject of management (brain or spinal cord) starts to work according to the natural resonance of the organ. For example,a team of researchers used the microcirculatory mode of REMATERA physiotherapy structural‐resonance therapeutic equipment and REKELSI physiotherapy electro‐stimulating equipment to treat the injured spinal cord of a patient with frequencies ranging from 5 836.09 Hz to 8 454.144 Hz and to 12 681.22 Hz and 93 seconds and demonstrated the opportunity to change the geometry and scope of the vascular bed of different organs and tissues [23].
Another method for reconstructive non‐ionizing EMR that can be applied for the remote restoration of the brain/spinal cord NT is the focused ultrasound effect. The ultrasound range of electromagnetic radiation is another instrument for the restoration of the damaged brain[25]. The lower border of the ultrasonic range involves elastic vibration at a frequency of up to 18 kHz. The upper border of ultrasound is defined by the origin of these elastic waves,which can spread only if the wavelength is much greater than the molecular free run (in gases) or interatomic distance (in liquids and solids). In gases,the upper border is ~106 kHz, and in liquids and solids ~1 010 kHz. Generally,frequencies up to 106 kHz are considered to be in the range of ultrasound. Higher frequencies are commonly referred to as hyper sound. Ultrasonic waves are inherently in the same as the audible waves and obey the same natural principles. However,ultrasound exhibits some specific features,which define its extensive application in science and technology: (1) Short wavelength. For the lowest ultrasonic range of most media,the wavelength does not exceed several centimeters. Short wavelengths provide for the propagation of ultrasonic waves. Near the transducer, ultrasound propagates in the form of bundles of beams,close to the size of the transducer. Falling on inconsistences in the medium,the ultrasonic bundle behaves as a light beam,suffering reflection, refraction,and scattering,which allows for the formation of audible images in an optically opaque media using purely optical effects (focusing,diffraction, etc.). (2) Short period of vibrations. The short period allows for ultrasound radiation in the form of pulses and the ability to perform accurate time selection for propagating the signals in the medium. (3) A possibility of obtaining high vibration energies. High vibration energies at low amplitude are possible because the energy of the vibrations is proportional to the square of the frequency. This allows for the formation of high‐energy ultrasonic bundles and fields, hence no requirement for large installations. (4) High acoustic currents are developed in the ultrasonic field. Therefore,the effect of ultrasound on the medium causes specific effects: physical,chemical,biological, or medical,such as cavitation,acoustic‐capillary effects, dispersion,emulsification,degassing,antiseptics,local heating,and many others[26].
Focused ultrasound fields have four important characteristics: (1) The field width is determined by the same angle of divergence as in the far field of a non‐focusing transducer. (2) The field is reduced only in the near field adjacent to the source before focusing. The far field cannot be focused. (3) The field width in focus is inversely proportional to the diameter of the transducer. (4) The field intensity reduces rather quickly away from the focal region. Therefore,the distribution of the focused field is limited. The beam width in the focus of the transducer or in the far field is determined as follows: W = ahZ/D,where h is a dominant wavelength of transmitted acoustic energy; Z—axial spacing from transducer; D—width of the transducer (diameter for the circular transducer); а is a constant that depends on the geometry of the transducer. For a circular or piston transducer a = 1.22 and for a rectangular transducer a = 1.0. Focusing is achieved with a plastic lens or phase shifting of the elements. Plastic lens are relatively cheap and yield good results. The optic system we used is produced by Schlieren, which produces ultrasonic waves that are made visible. With strong focusing,the field concentrates in focus and does not extend very far beyond. On the contrary, if the focusing of ultrasound transducer of the same diameter is weak,the near field is distributed at a rather long distance. Focusing of the ultrasound beam in an electronic phase shifting system is achieved through the combination of spherical and linear spatialtemporal interrelationships of the impulses,received by the transducer. Such electronic processing of the signals results in the focus of the ultrasound field at a specific distance,and the field is distributed at a specific azimuthal angle[27].
Therapeutic ultrasound can be subdivided into low‐intensity and high‐intensity ultrasound. The main aim of the application of low‐intensity ultrasound is for the heating or induction of non‐heating effect without accompanying tissue damage as well as the stimulation and acceleration of normal physical reactions. However,at higher ultrasound intensities the objective is to cause selective destruction of tissues. The first category encompasses most applications of ultrasound in physiotherapy and some types of cancer therapy,while the second includes ultrasonic surgery[25].
The novel solutions in the application of ultrasound in the treatment of nervous disorders are technologies associated with magnetic resonance guided focused ultrasound (MRgFUS). Due to the MRgFUS technology a new field has appeared,known as non‐invasive functional neurosurgery. Gavrilov[26] thinks that this interest in focused ultrasound was revived quite recently,when Hynynen et al.[28] demonstrated that ultrasound could penetrate the skull. It has been proven that low intensity ultrasonic waves,affecting deep areas of the brain,can stop the uncontrolled twitching of the extremities and the head,treat essential tremors,tremors in Parkinson’s disease,Meniere’s syndrome,and activate neural networks of the human brain.
In July 2006, the 3 Tesla MRI guided system ExAblate was installed in the university hospital of Zurich, Switzerland. This system provides for pinpoint focused ultrasound treatment of the conducting pathways in the brain. The first patients to receive non‐invasive Tran cranial MRgFUS were patients suffering from neurogenic pain,Parkinson’s disease,and epilepsy. By 2009,the first ten patients had received the treatment. MRgFUS is a contemporary alternative to surgical removal of the tumors and organs. It is a non‐invasive outpatient procedure that can be easily adjusted and repeated as many times as necessary. For the ablation of brain tumors without craniotomy,a special thousandelement, helmet‐like transducer with an external cooling system and stereotaxic frame has been developed. Several patients with glioblastoma have received MRgFUS ablation of tumors in Brigham and Women’s Hospital (MA,USA). The first results were positively evaluated. The clinical trial continues at 4 treatment centers (MA,VA,USA; Canada and Israel)[27].
US researchers from Columbia University have demonstrated that FUS with a near critical intensity causes no irreversible changes in the structure of the brain,can considerably activate and synchronize neural networks of the brain. The interest in this method keeps growing throughout the world,since its appearance in 2004. So,in the US and some European countries the focus of ultrasound is used to treat pains resulting from metastases in bones and joints, and to treat fibroadenoma,breast cancer,prostate cancer,and many other neurological diseases,particularly the essential tremor in Parkinson’s disease.
The effect of ultrasound application to the brain causes changes to BBB permeability. This neurobiological phenomenon was demonstrated by the Perfusion Technology in Andover (MA,USA). The BBB is the natural protection of the brain tissues from penetration of potentially harmful agents. However, the BBB prevents the penetration of pharmaceuticals, regulatory cell systems,and stem cells to the brain and spinal cord for therapeutic purposes. Using this method to alter the permeability of the BBB is simple and cheap according to Perfusion Technology. Instead of opening the BBB at a single point,the method of ultrasonic perfusion applies a specially designed headset to expose the entire brain to low‐intensity ultrasound waves for an hour‐long treatment session. The headsets of the Perfusion Technology spread ultrasonic waves throughout the brain and anti‐cancer agents of other large molecules reduce in size and can cross the blood brain barrier[27].
Therefore,it is obvious that contemporary medicine will find a way to exploit the described methods of ionizing and non‐ionizing electromagnetic radiation to treat pathologies of the brain and spinal cord. The methods of the exposure and appropriate medical equipment are approved for clinical application in Russia and the majority of high‐income countries (USA, Great Britain,Canada,Germany,etc.).
However,each of these methods of remote exposure is applied to a limited number of pathologies of the brain,in a fragmentary and isolated way depending on the character of the tissue injury,such as tumors or tremor,as the method has very specific local neurobiological effect on the NT of the brain and spinal cord. Meanwhile,the well‐known systemic neurobiological mechanisms of the combined effect of different types of radiation are ignored,which can provide a programmed restorative effect on the NT.
3.5 The subject matter of this technology This technology does not offer a final solution for the treatment of neural and mental diseases,but further expansion for the use of IR and non‐IR of EMR in the reconstruction of the human brain and spinal cord demands a reduction of potential harm resulting from possible complications of the clinical application of EMR. We think that the main difficulties and reservations about the radio‐sensitivity/radio‐vulnerability of the brain under the exposure of low doses of ionizing EMR can be overcome by simultaneous local application of low doses of different types of electromagnetic effect NT cells in the human brain and spinal cord. This new aspect of consecutive and combined application of ionizing EMR and other types of non‐ionizing EMR for the restoration of human brain will allow us to avoid many complications resulting from the isolated use of these technologies in clinical practice and to implement the strategy to intratissular reconstruction of the brain/ spinal cord. The principle of consecutive and combined effects of applying different types of EMR on the NT in the human brain and spinal cord was taken as the basis for the proposed technology. The combined exposure of the NT to ionizing and non‐ionizing EMR allows for the necessary combination of the neurobiological effects in the site of reconstruction. For example,the combination of IR and focused low intensive ultrasound in specific point of NT can cause synergetic and inter‐correlating neurobiological effects: (1) Temporal permeability of the BBB for bioactive agents,stem and progenitor cells of the bone marrow and tissuespecific stem cells. (2) Creation of the inflammatory concentration gradient in the site NT reconstruction for targeted transport of the SCs and PCs. (3) Reduction of negative side effects of the selective application of the low doses of IR on the cells of NT of the brain and spinal cord. (4) The combined effect of SRT and FUS promotes microcirculation at the restoration site for the damaged brain due to general systemic microcirculatory effect of the SRT on the NT of a whole brain and amelioration of the local microcirculatory effects by the focused ultrasonic massaging effect on the NT and the elimination of local angiospastic and angioparalytic influences on the micro‐capillaries of the disordered vegetative supply of veins and arteries in the site of brain[29].The simultaneous combined action of low doses of IR and SRT in a rehabilitation regimen for damaged NT of the brain and spinal cord contributes to: (1) Bioelectrical activation of brain without postradiation molecular‐biological effects of IR application. (2) Elimination of systemic pathological connections in the damaged NT of the human brain/spinal cord by IR and the imposition of SRT resonant‐wave frequencies of the physiological range for restoration of NT function.
Contemporary medical literature describes experimental evidence of positive and mutually correcting applications of different types of electromagnetic radiation that for several reasons have not found their clinical application. For the first time,the idea of a positive effect on biological systems that have been exposed to ionizing radiation by other non‐ionizing electromagnetic fields of weak or non‐heating activity, which in this context acquire a new meaning of the information signals,was described by A. S. Presman,a Moscow biophysicist,in a book entitled "Electromagnetic Fields and Living Nature"[17]. It is well known that the unfavorable effects of average and low doses of ionizing radiation on the human health can be neutralized by the action of non‐ionizing electromagnetic waves from an extremely high band[30] and structural resonant electromagnetic properties[23]. The positive influence of non‐ionizing EMR on the side effects of ionizing EMR can be associated with the biological resonances of the EMR. In addition,changes are the modulation frequency of the EMR,which is the information frequency that carries the major part of the appropriate information. EMR modulation results from changes in the amplitude,frequency,or phase of harmonic oscillation according to the specific pattern to introduce necessary information into the oscillatory process. The transfer of information with the help of electromagnetic waves due to their modulation is possible only in the low frequency band corresponding to the frequency band of the functional systems of the body (from 1 to 10 Hz). Imposition of the physiological resonant frequencies of the norm on the brain tissue that was damaged by the ionizing ER by the methods of SRT corrects the negative postradiation molecular‐biological effects of low doses of IR in the tissue and renders the effect almost harmless, while in the combination with Χ-ray radiation or antitumor preparations with the EMW of non‐IR function as the protector[30].
There is the other no less important aspect of the simultaneous combination of EMR exposure in the brain. The combined application of low doses of different types of ionizing EMR with FUS allows the simultaneous purposeful management of different postradiation neurobiological effects. For example,we have already noted that the combined,simultaneous application of low‐frequency FUS with low doses of IR exposure on the reconstruction site of the brain allows for two important neurobiological phenomena: (1) Focused ultrasound increases super‐selective permeability of the BBB for HSCs and/or mesenchymal SCs in the site of reconstruction. (2) Low doses of IR will establish an area of aseptic inflammation and,hence,the appropriate concentration gradient of cytokines and inflammation factors that provide for the targeted migration of stem and progenitor cells from peripheral blood and bone marrow to the site of reconstruction. The intensity of every neurobiological phenomenon can be regulated by additional methods of imaging (contrast‐enhanced MRI,NT thermometry, PET,etc.). Therefore,the combination of stereotaxic simultaneous effect of FUS and IR in the brain restoration sites solves several important tasks of targeting SCs and free access to the site of injury across the BBB with the consequent restoration of protective functions of the BBB.
The combined use of non‐ionizing EMR of low intensity (SRT) with low frequency FUS contributes to the quick restoration of life‐sustaining processes in the damaged tissues[30]. This is the result of enhanced proliferative activity of hematopoietic stem cells (HSCs), thus leading to mitotic activity of the bone marrow cells. The effect of low intensity EMR on the cells of bone marrow was studied in vitro[31] and showed that low‐intensity,non‐heating EMR is beneficial for the HSCs of cryopreserved bone marrow,contributing to the viability of lethally irradiated recipients following myelo‐transplantation and can be one of the methods used to increase the regenerative capacity of the cryopreserved bone marrow. The research team of Govallo VI in the Central Research Institute of Traumatology and Orthopedy (Russia) together with scientific‐production association Istok (Russia) showed in vitro that the human lymphocytes and fibroblasts produce a phytokine that promotes growth and functional activity of analogous cells when exposed to EHF waves[24].
The simultaneous application of electromagnetic radiations of SRT and FUS in the site of reconstruction can considerably improve the general synchronization of components of the damaged tissue due to activation of nerve cells,massaging the effects into the NT through the application of low‐frequency FUS and imposition of physiological rhythms to the whole brain and to the site of reconstruction by the appropriate modes of SRT.
Therefore,certain combinations of EMR that simultaneously or consecutively affect the site of injury in the brain/spinal cord NT,can produce specific and rather stable effects that can be used for specific purposes of the NT reconstruction. The combined radio‐reconstructive effect of these types of radiation can realize all multi‐functional changes in the NT of the brain/spinal cord that are necessary for its reconstruction in a remote way,and not surgically as described in the prototype technology. This remote selective and combined restorative multi‐wave effect of different types of EMR on the NT in the recipient’s brain is a method of remote non‐contact mediated radio‐bioengineering or radio‐neuroengineering.
Technically,the proposed method of treatment of nervous and mental diseases solves the task through the restoration of the damaged NT by purposeful means through a program of focused exposure in the brain,by initiation of specific neurobiological effects of certain radio (IR) or wave (non‐IR) effects (FUS or SRT),as well as by the combination (IR+FUS,IR+SRT, SRT+FUS) of multi‐level and multi‐wave stereotaxic effects on the NT by providing for the appropriate therapeutic molecular‐biological and neuromorphic effects.
Hence,the goal of this technology is the development of basically new methodological and technological approaches in the bioengineering and tissue engineering of the human brain NT,based on the remote stereotaxic non‐contact reconstruction of the damaged NT by targeted combined effects of different EMRs, as well as the development of the helmet‐like construction for stereotaxic clamping of the head and rigid attachment of the transducer units of registration and targeted action of the EMRs. Our innovation resulted in the development of a new method to treat nervous and mental diseases,using remote non‐surgical and non‐invasive radio‐bioengineering plasty of the NT of the brain/spinal cord by the combination and simultaneous application of low doses of IR and low efficiency of the radiation of the brain by different types of non‐IR of EMR.
The technology was implemented on the basis of highly technological method of non‐contact reconstructive‐restorative multi‐wave combined electromagnetic effect (IR + FUS,SRT + FUS,IR‐SRT) on the injured NT of human brain and spinal cord. Restoration and reconstruction of the injured NT was achieved due to the duration and intensity of the required neurobiological effects.
We would like to repeat important evidence that necessary (program) neurobiological effects in the NT were induced by parallel (simultaneous) or consecutive combinatory focus action of different types of IR and non‐IR of the low intensity EMWs with different wavelengths. Thus,we trigger specific restorative molecular‐biological mechanisms: micro‐circulation or aplasia of micro‐vascular bed,regeneration or degeneration of nerve cells,activation or depression of the speed of conduction of the nerve impulses,homing and pathotropism of cell systems,aseptic inflammation or radio necrosis,etc. These neurobiological effects in NT,if used in an algorithmized and program way, led to the multilevel restoration of the main elements of NT,due to improved microcirculation in the site, activation of regulatory properties of the SCs of bone marrow,restoration of autonomous vegetative supply and normalization of the biorhythms of NT functioning. As a result,the quantitative and qualitative restoration of the cell composition (neurons,oligodendrocytes, microglia,fibers synapses,etc.) in the site of injury,management of the BBB permeability,vascular remodeling of the site of reconstruction (change of vascular geometry and size of micro‐vascular bed) is achieved,the regulation of synaptogenesis in the damaged NT and re‐modulation of autonomous vegetative supply of the NT of the site of injury (appropriate change of the tone of sympathetic and parasympathetic nervous system) is activated, and the main system‐forming components of NT are synchronized.
Hence,the proposed bioengineering method of the treatment of the brain disorders provides remote intratissular restoration of the multifunctional structure of the damaged NT of the human brain in nervous and mental diseases,brain traumas and spinal cord traumas without neurosurgical or low‐invasive interventions of radiosurgery and excludes direct contact with the NT.
3.6 Stereotaxic helmet‐like equipment for radioneuroengineering To illustrate and to examine the therapeutic opportunities of the proposed principle of combined distant radio‐bioengineering action (SRT+FUS) on the damaged NT of the human brain,we proposed the demo version of the stereotaxic equipment for simultaneous multi‐wave action,where the diagnostic and therapeutic transducer units of non‐IR of EMR are installed and connected to a standard therapeutic ultrasonography and standard equipment for STR. For these purposes,we used a well‐known method of stereotaxic navigation to the subcortical structures of the brain that was worked out on the basis of the available stereotaxic equipment.The stereotaxic surgery is the combination of the means and methods with the help of which any practical task of low‐invasive surgical access to any regions of the brain is achieved on the basis mathematical calculations and significantly depends on correct understanding of the geometric properties of the Χ-ray image. The stereotaxic method,or,stereotaxy (from Greek stereo- meaning "three‐dimensional","solid", and -taxis meaning "arrangement","order") is the combination of the means and calculations that permit high precision introduction of cannula (electrode) into provisionally determined deeply located structure of the brain or spinal cord in order to treat it under the control of special equipment and methods of functional and Χ-ray management. As far as our aim does not involve surgical operation on the NT,the priority was given to detection of the angulation and points in the brain for multi‐wave action from different types of ultrasonic transducer units of EMR.
The main principle of stereotaxic surgery is correlation of the relative system of reference of the brain with the system of reference of the stereotaxic equipment[32]. For us,the relative system of reference of the restoration sites in the brain was the marks done by the radiologist on radiosurgical equipment,and the assignment of coordinates for non‐IR (FUS and SRT). For the simultaneous focused electromagnetic IT and non‐IR EMW targeted at specific sites of the damaged NT,we used the stereotaxic equipment adapted to the task of NT reconstruction,where the main principle of stereotaxy is retained. Despite a great variety of stereotaxic apparatuses,and,accordingly,of stereotaxic calculations,the correlation of the system of reference of the brain with the system of reference of the stereotaxic equipment relies on one principle of three‐dimensional orthogonal and polar projections. As Abrakov[32] notes,the seeming variety of the methods of these calculations is not beneficial and only disguises the integrity of the general principles. Cartesian coordinates imply calculation in three orthogonal axes,so that we can exactly determine the magnification of the object in the parallax effect and to repeatedly install the apparatus in the same way,if the intervention has 2 stages. However,the apparatuses that use Cartesian system of coordinates have the drawbacks: complexity of the construction,difficulty in mounting the frame and complex time‐consuming calculations. The stereotaxic apparatuses based on the system of polar coordinates are more widely used. The principle is the following: an electrode‐cannula is introduced into the brain in the direction to the point at specific angles. The angles are determined with the help of the lines drawn from the tip of an electrodecannula that was introduced deep into the brain at an image in both projections[32].
From the practical point of view,all existing apparatuses can be subdivided into two groups: (1) The apparatuses of a relatively simple construction that are mounted in a small burr hole in the skull. Mounting of these apparatuses does not need Χ-ray control and is done according to external guide marks. (2) The apparatuses of complex construction and big size where the head is framed under the Χ-ray control with the help of the screws in the skull.
For remote restoration of the brain,we think practical to use the second type of stereotaxic apparatus that was used for radio‐neuroengineering. Apparently, complex and cumbersome apparatuses of the second type require much time for calculations and mounting, and are inconvenient in the surgery room. However, for the purposes of the radio‐neuroengineering and remote neurorestoration and reconstruction of the damaged NT,they are quite convenient and safe, and can be widely used after appropriate update and simplification. Application of these apparatuses renders the process of radio‐engineering quite mobile. The apparatus can be established in the medical treatment room or in the physiotherapy rooms for SRT and FUS, and can be used in the radiosurgery room of radiotherapeutic department. However,it is clear that accuracy of the apparatus cannot be sacrificed to the simplicity and convenience of use. Accuracy of the multi‐wave focus effect on the subcortical structures is achieved by calculations and modeling at the computer‐guided radiotherapeutic (radiosurgical) stereotaxic apparatus that provides for necessary effect of IR at the site of reconstruction. The transducer units of ultrasound are installed on the clamps of stereotaxical apparatus and positioned at specific angles to the skull,according to the marks that provide focusing of the ultrasonic beams in the site of neuroengineering plasty of the brain; while,the inducers of structural‐resonance effect are mounted on the frame of stereotaxic apparatus in the forehead and occipital areas. To monitor the efficiency and safety of the procedure,the helmet is mounted on the head of the patient to set the electrodes for the registration of the bioelectric activity of the brain. Figure8 shows the photo of the proposed stereotaxic equipment with the transducer units for multi‐wave focus ultrasound effect.
3.7 Technological stages of radio‐neuroengineering The remote radio‐neuroengineering can follow the stages that are analogous to the interventional surgical bioengineering presented in the prototype technology. However,the technical implementation of the method must be based only on the up‐to‐date information radio computer technologies and should not involve surgery. We think that the technology of the noncontact radio‐neuroengineering establishes a new paradigm,almost a new way of non‐contact surgery and can become one of the ideas that will change the world.The biotechnology involves all stages of restoration of the damaged brain as in the prototype technology, but at a new technological level of multi‐wave electromagnetic action. In the proposed invention of the therapy of nervous and mental diseases the stage of design is aimed at the diagnostics of the sites of injury in the brain. In this case,it is important to analyze morphological damage and detect localization of the areas of functional injury in the brain and spinal cord. To evaluate the size of reconstruction,it is necessary to gather as accurate data of the type of injury of the NT,as it is only possible. These data can be provided by high‐resolution MRI of the brain that allows the study of resonant‐wave characteristics of the inductivity of the NT in the site of injury.
The data of the analysis of metabolic changes in different areas of the brain/spinal cord can be received from PET. Fusion of the PET images with the CT permits accurate coupling of the evidence of metabolomic disorder in the site of injury and its localization in organs and tissues. Therefore,the technology of the fused PET/CT opens new perspectives in the diagnostics of morphofunctional changes and their location in the anatomical formation of the brain. We can receive the data about magnetization of NT as a functional characteristic of the NT damage using magneto-encephalography (MEG). The data of threedimensional mapping of EEG provide us the evidence of the location of bioelectric activity of the brain cortex.
Program fusion of these data in the tables of bio information mapping of the brain with the data of MRI and CT gives us integral characteristic and maximally verified biological information of the personalized data that can be used by contemporary IT‐technologies and methods of mathematical modeling. Hence,these contemporary data of the imaging of the human brain help plan our restorative efforts in the neuroengineering, determine the main directions and information levels of the reconstruction of the brain and spinal cord and to evaluate the scope of requisite biomaterials and instruments. The specialized software for multilevel fusion (multi‐fusion) of the data of MRI,CT,PET,EEG mapping and MEG will produce a table of the parameters of different brain areas,so that it is possible to compare it with the table of the norm and to detect the injuries and functional disorders that have been missed by the physician during the visual analysis.
The obtained multi‐level data about the condition of the patient’s brain must be provided at contemporary carriers (CD,DVDs,flash drives,etc.) for the bioinformation analysis and they must be recorded in DICOM standard. The requirements for the research at this stage are the following: (1) No less than 1.5 Tesla MRI. (2) MRI tractography of conduction pathways in the site of injury of the brain/spinal cord. (3) MRI angiography of the brain vessels. (4) PET of the brain or a whole body,for spinal cords the standard radioisotopes of glucose PET must be done. (5) No less than 32 slice spiral CT of the brain or the spinal cord and spine. (6) Cerebral EEG mapping must be on the EEG equipment with the software for 3D local modeling of the bioelectrical activity of the brain/spinal cord. (7) MEG of the brain with 3D modeling.
The time period between different imaging tests should be not more than a week. All imaging tests that were done at the preparatory stage for the examination can be used at the next stage to monitor the effectiveness of the therapy. The imaging data can be fused into 3D maps of the brain with the help of the Multimodal fusion 3D software of the Cyberknife robotic radiosurgery system or similar systems for stereotaxic radiotherapy of other manufacturers. With this approach a three‐dimensional multi‐level mapped model of the information structure of the damaged NT of the brain/spinal cord of the nerve or mental disease case can be represented as the set of the tables of local data,that correlate them with anatomical formations in the brain so that the personalized functional 3D map of pathological changes and damages the NT of the specific case. Such a 3D map can be the basis for the marking and stereotaxic targeted therapeutic radio‐bioengineering effect of IR on the brain or spinal cord. This stage of the proposed treatment of nervous and mental diseases can be illustrated by the clinical case of the patient B. Figures 2-7 represent the data of different stages of the technology of multilevel fusion of the data of computerized tests.

|
| Figure 2 a–e. 3 Tesla MRI of the brain of patient B. |

|
| Figure 3 a–c. MRItractography of the conducting pathways of the brain of patient B. |

|
| Figure 4 CT of the brain of patient B. |

|
| Figure 5 a–c. PET scanning of the brain of patient B. |

|
| Figure 6 a–h. Fusion of CT, MRI tractography and PET of the brain of patient B. |

|
| Figure 7 a–c. Images of 3D multimode reconstruction of the nervous tissue of the brain of patient B. |
At this stage of the technology the marks for further radio‐bioengineering effect on the brain are made on a standard radio therapeutic (radiosurgical) stereotaxic system with due account for a 3D map of the case history.
On the basis of the marks,the "radio marks" are made on the scalp to mount the stereotaxic apparatus on the patient’s head for the targeted stereotaxic effect of the IR and non‐IR of EMR on the brain,and the main vertical and horizontal angles and azimuths are detected to provide for stereotaxic application of the IR,SRT and FUS of the specialized transducer units in the clamps of the stereotaxic apparatus Figures 8(a) and 8(b).

|
| Figure 8 The stereotaxic apparatus used for remote radio‐neuroeng ineering multi‐wave (structuralresonance and ultrasonic) focused electromagnetic under the control of EEG cerebral mapping. a – front view; b – rear view. |
Without any doubt,the correct,highly technological and the most reasonable solution of all tasks of radioneuroengineering for the remote restoration of the damaged NT of the brain would be the development of a new class of specialized medical equipment on the platform of the standard stereotaxic radiosurgical system,in which the stereotaxic IR effect will be supplemented by non‐IR EMR (focused ultrasonic effect and structural‐resonance effect). The combination of the transducer units of FUS,CRT inductors and appropriate equipment for the treatment on the basis of stereotaxic radiosurgical technological platform allows for different combinations of the therapeutic effect of IR and non‐IR in a programmed way.
The well‐known technologies of the wave nonionizing electromagnetic effect on the brain are analogous to the Χ-ray stage of the vascular remodeling in the prototype technology. Two strategies can be realized,depending on the pathogenesis of the brain disease and specific tasks of the stage: (1) devascularization of the site of injury (in tumors, micro‐aneurisms,malformations,hemorrhages, etc.),and (2) hypervascularization of the site of injury (ischemia,atrophy,demyelination,etc.). Destruction of the supplying vessels by the MR‐guided focused ultrasound is a ready‐made solution for devascularization as the first stage of the complex therapy on a FUS‐MRI system[26]. Ablation of the vessels by the focused ultrasound provides total occlusion of the tumor or neoplasm supplying arteries. Other strategy of remodeling of the vascular bed aims at the expansion of its geometry and increase of blood flow is implemented by opening of micro‐capillaries and micro‐venules in the site of injury. It is achieved in remote hypervascularization and microcirculatory remodeling effect on the brain by the electromagnetic SRT equipment[23] and FUS standard equipment for ultrasonic therapy. The authors of the SRT proposed to use the equipment for electromagnetic therapy in microcirculatory mode. The equipment consists of a high‐frequency reference generator,a scalar,a switch,an operating device with controlling elements,modulation frequency indicator,carrier frequency indicator,signal conditioner,output amplifiers with mode control switch,inductors and inductor current indicators,the output of the reference generator connects with the input of the scaler,the first output of which connects with the first output of the switch, and the second output of the scaler connects to the input of the operating device,the first output of which connects to the second input of the switch,the second output of the operating device connects to the modulation frequency indicator,the third output of the operating device connects to the carrier frequency indicator,the outputs of the switch connect to the inputs of the signal conditioner,the outputs of which connect to the inputs of the output amplifiers,the outputs of which connect to the inductors and inductor current indicators. The scaler of the apparatus is multiple‐stage. Kuzovlev and his team[23] demonstrated the microcirculatory effect of the EMWs on human tissue in experiment,as they developed the already known method of remote effect on the brain patented as "The Method to Affect a Biological Object"[24],according to which an organ or tissue is stimulated by electric current or alternating magnetic field,and the frequency range of the stimulation is calculated according to the empirical expression. The method was updated and is known as structuralresonance therapy (SRT). The kernel of SRT is in the involvement of the structures of an organism into resonant "oscillation",and the damaged structures that have an asymmetric moment go out of balance, the pathological ingredients withdraw to the general system of homeostasis,and relieved healthy tissues remain unchanged. The resonant,highly effective frequencies of therapeutic signal were empirically searched for under the control of clinical‐instrumental methods of analysis of the disease follow‐up during 25 years. The SRT is based on the well‐known standard value of the fluctuation rate of atomic extraterrestrial hydrogen,a primary reference information generator of the development of all types of physical structures, which is 1 420 817 336 Hz. To construct initial points (left row) of the bifurcation of rhythm cascades the rule of the octave with coefficient 2 is used,and to construct last points of bifurcation the golden section rule[33] is used and the value of the initial point is multiplied by 1.5 or the sum of the values of the initial frequencies of the same rhythm cascade and the previous (with the smaller frequency value). Difference in the values of the frequencies in the bifurcation points of rhythm cascades in SRT varies only from 3.7 А% to 4.7 А%.
The SRT for microcirculation in the brain is implemented using different types of equipment,for example: (1) Electro‐stimulator: KELSI and RADOMYS using current‐conducting rubber knitted graphitized cloth or silvered polymer to affect mucosa. (2) Apparatus for electromagnetic therapy that provides non‐contact effect with the help of the inductors from belt‐like multicore cables.
As far as the pathology,as a rule,violates the evolutionary rational connections between different organs and systems and,consequently,it is necessary to consecutively "fix" ever level of organization, known by its rhythm cascades,the pathology of which was detected in conventional diagnostic methods. When the method is implemented,it is possible to use a so‐called "scanning" mode,when the carrier frequencies that start from minimal,go through all possible biorhythms of structural‐functional units to cellular and sub‐cellular levels and return to the initial, are conducted through the envelope frequency,which is characteristic for specific level of organization.
The standard ultrasonic pencil‐like transducer units applied for the ultrasonic diagnostics of the head and neck vessels in neurosurgery were used to model FUS, affecting the site of injury. The ultrasonic transducers, attached to the stereotaxic apparatus and oriented on the intracerebral focus action,were connected to the standard equipment for ultrasonic therapy and produced ultrasonic effect. A universal ultrasonic therapeutic apparatus UST‐107F with microprocessorbased control is meant for the treatment of different disorders of peripheral nervous system. The specific features of the apparatus are smooth regulation of intensity and more accurate dosing of radiation. The apparatus is AC powered: voltage is 220±10% V/50 Hz. Watt consumption is no more than 45 W; frequency of ultrasound is 0.88±0.1% MHz; effective area of the radiators in cm2: 0.88 1.03F‐1; 0.88 1.05F‐1; 0.88 4.04F‐4; operating mode is continuous and impulse. The regulation of output power is step by step. The intensity of ultrasonic oscillations is by the steps from 0 to 1 W/cm3, with 0.1 steps. Pulse repetition rate is 50 Hz. The following radiators were used to model stereotaxic focused effect: IUT 0.88 05.10F,IUT 0.88 1.06F,IUT 0.88 1.090,IUT 0.88 2.07S,IUT 0.88 2.08U. The standard ultrasound gel for better adherence of the ultrasonic transducers with the scalp was used. The FUS procedure lasted from 10 to 30 minutes and coincided with SRT.
The third stage of the bioengineering reconstruction of the brain in the prototype technology,known as the stage of cell transplantation,consisted in surgical transplantation of the cells to the site of injury. The inherent neurobiological features and migration patterns of autologous HSCs and PCs allowed for targeted delivery of the SCs and PCs. In other words, we did not attract them artificially (magnetic induction, antigen‐antibody mechanism,vector immune liposomal delivery,etc.),but used genetic mechanisms of HSC pathotropism that underlie self‐regulation and sanogenesis. The proposed method relies on the fundamental neurobiological molecular‐cellular phenomena of mammalian SCs and PCs (homing,pathotropism,cell adhesion and by‐stander effect). For that the stimulation of the bone marrow with granulocyte colony‐stimulating factor (G‐CSF) for 5 days to induce the exit of HSCs and mesenchymal SCs and PCs into peripheral blood flow was used along with several basic phenomena of interaction of different types of waves of IR and non‐IR of electromagnetic effect with different types of the cells of NT.
The stage of cell transplantation was implemented as the remote targeted migration of SCs from bone marrow to the site of injury of the brain/spinal cord, using a conventional technique of HSCs harvest used for bone marrow transplantation and treatment of the chronic spinal cord injury [12]. The main methods of cell delivery and cell intervention into the lesions of the brain and spinal cord are the mobilization of HSCs and PCs to the systemic blood flow by G‐CSF, and intravenous or intrathecal cytotransfusions of cryopreserved HSCs,intravenous or intra‐arterial infusions of haploidentical mesenchymal stromal SCs (MSSCs) of bone marrow or autologous neural SCs. It was proved[34] that after 4 days of G‐CSF administration a rather large number (30×106-50×106) of white blood cells circulate in blood,and 1%-1.2% of them are hematopoietic and mesenchymal SCs with CD34+ CD45‐ markers. This period of restoration implied development of a targeting vector for the autologous SCs and PCs delivery and establishment of the conditions for their migration to the site of injury,as well as the achievement of maximal concentration of SCs and PCs in the sites. At this stage,a neurological or psychiatric patient received G‐CSF for 4 days, physostigminum intramuscular twice a day under control of daily blood tests.
The SCs and MSSCs of bone marrow promote restoration in the site of injury of the brain or spinal cord in case: (1) They are mobilized to peripheral blood by G‐CSF and their concentration in peripheral blood reaches its peak by day 5. (2) They are administered to the brain/spinal cord parenchyma by systemic intrathecal, intraventricular or intra‐arterial transfusion. (3) They demonstrate their inherent properties: ① arrive to the pathological area in the NT independent from the genesis of the pathology (inflammation,hemorrhage, ischemia,tumor, etc.),② adhere to pathological cells of the site of injury due to cell adhesion,③ provide regulatory,neurotrophic or stimulating effect due to bye‐stander effect,and ④ the damaged cells in the NT can be restored by their replacement or fusion with them or by establishing new synaptic contacts between the transplanted donor cells and nerve cells of the recipient[14].
At day 6 the leukapheresis on COBE Spectra system is performed and the mobilized stem cells of bone marrow are harvested,standardized and cryopreserved. This stage of remote transplantation of the cells is to provide free super selective access of circulating SCs from peripheral blood to the specific sites of NT reconstruction that were determined at the stage of design. Under the standard conditions of the brain and spinal cord functioning,the BBB prevents the access of HSCs,PCs,and MSSCs to NT from peripheral blood.
To overcome this natural defense and to provide the access of the cells to the NT parenchyma the low doses of ionizing EMR were used. The low doses of ionizing radiations combined with FUS were applied to promote the regeneration in the site of brain/spinal cord reconstruction,to temporally open the BBB for HSCs,PCs and MSSCs and their targeted migration, to destabilize established pathological intercellular connections in the NT,to induce intercellular genetic instability in the NT cell systems and to change inductivity of NT in the site of reconstruction.
According to the available evidence[18] and our own research,the threshold doses of cerebral radiation are the doses of 0.1-0.3 Gy for children,and radiationassociated neurobiological effect in adults were observed >0.15-0.2 Sv. Dose‐dependent neuropsychiatric, neurophysiologic and neuroimaging irregularities were observed after radiation in the doses >0.3 Sv,and neurophysiologic and neuroimaging markers in the doses >1 Sv.
Therefore,the allowable total dose of IR must be less than or equal to 0.3 Sv. The dose of IR can provide genetic instability of the nerve cells in the site of reconstruction and transitory (to 6 hours) permeability of the BBB for cellular mononuclear systems of blood (HSCs,PCs,MSSCs),monoclonal antibodies and biologically active molecules of the proteins from peripheral blood[35]. The use of the radiosurgical systems (CyberKnife,GammaKnife and other) for local IR of brain/spinal cord NT allow for super selective focus of the dose directly in the sites of the brain reconstruction. The IR applied to NT of the brain and spinal cord with the help of these radiosurgical systems at the peak concentration of HSCs,PCs and MSSCs in peripheral blood will provide their free exit through capillary network in the sites of stereotaxic radiation[36]. To increase permeability of the BBB,the ozonized 0.9% saline is intravenously administered or FUS is applied. These procedures enhance permeability of the BBB for one hour and will significantly contribute to the saturation of the tissue with oxygen in the reconstruction site improving temporal permeability of the BBB. The delayed effects that contribute to the permeability of the BBB after IR and FUS will be observed after multi‐wave effect,build up in an hour or an hour and a half and last for about 12 hours, contributing to further access of stem and progenitor cells to the nervous system and cellular saturation of the sites of the brain reconstruction.
The next stage of the NT reconstruction will be the stage of correction of vegetative supply. The main vegetative components of tissue supply,for example, the bodies and synapses of the nerve cells located in the vegetative ganglia of sympathetic and parasympathetic nervous system belong to the most vulnerable to the pathological process in the NT. Degeneration and shrinkage of the nerve cells,such as fat degeneration of neural structures in vegetative ganglia that was first described by Claude Bernard became the business card of any pathological process in the brain tissue[11]. As we noted in the prototype technology the vegetative supply was corrected in a rather primitive way: (1) Complete disconnection of sympathetic nerve supply area by sympathectomy. (2) Partial disconnection of sympathetic nerve supply by sympathetic block of stellate ganglion on the side of the injury (by 1% Novocain or Lidocain) or by transplantation of the preparation of nerve cells. (3) Transplantation of neural stem cells into sympathetic ganglia.
In the current invention we have achieved the same sympathetic and parasympathetic effects by the specialized mode of SRT. To correct predomination of the sympathetic nerve supply,the mode "sympathetic nervous system" (SRT frequencies number 7‐13) was used; and for predomination of the parasympathetic nerve supply in the clinical picture the mode "Parasympathetic system——Brain Cortex" was used (SRT frequencies number 14‐15). Simultaneously with SRT for vegetative nerve supply the mode of complex simultaneous FUS of the phonophoresis type was applied to the area of stellate ganglion.
The next stage of the remote bioengineering reconstruction of the injured brain and spinal cord was the stage of dynamic integration of somatic and vegetative components that was implemented in the use of FUS and SRT in the destabilization modes. Destabilization mode of SRT corresponds to the envelope frequency of 194 Hz; carrier frequency was 12 500 Hz,75 000 Hz,and 150 000Hz. These SRT effects led to the disintegration of the site of the NT reconstruction,and further synchronization of the elements of the elements was achieved due to FUS. To date,the system‐forming and regulatory effects of ultrasound for the restoration of the NT are well known.
The stage of rehabilitation in the technology of remote radio‐engineering represented rehabilitation of the functional condition of the damaged NT,and not the physical rehabilitation of the body of the patient. It was realized by SRE of the brain NT and stimulating FUS. As far as the therapeutic signal of SRT is based on the biologically grounded code of morphogenetic field,its application is safe and does not demand special training of the operator. SRE exposition not only has no restrictions,but,on the contrary,the longer and oftener the sessions are,the quicker the patient restores,especially,in the acute phase and poor condition. Non‐contact electromagnetic effect (the general spectrum of therapeutic signal frequency range from 0.04 Hz to 50 000 Hz) is beneficial in the cases when the normal regulation needs restoration and the main biorhythms must be tuned. The injured NT can be rehabilitated by contact percutaneous effect of electric current (the general spectrum of therapeutic signal frequency range from ≥ 200 Hz) and has the benefit in the therapy of the organs that are located deeply, organs that have no spontaneous biopotential activity, for dystrophy or inflammation of the facial nerve,neuritis,radiculitis,neuralgic pains,metabolic syndromes of various genesis,in the complex therapy of benign tumors (under accurate control of the specialists). The disadvantages of local relaxing and sedating effect of SRT can be compensated by local effect of the FUS,thus,considerably enhancing rehabilitative restorative properties of the combined treatment.
4 The results and discussion The effectiveness of the technology of regulation of the NT was evaluated in 30 cases of severe organic diseases of the nervous system: 10 cases of chronic traumatic brain injury,15 cases of chronic spinal cord injury,2 cases of amyotrophic lateral sclerosis and 3 cases of multiple sclerosis. Detailed clinical data,the results and discussion will be provided in a separate submission. The method of radio‐bioengineering was tried under clinical conditions and the complex technological program order of classical methods of bioengineering (mobilization of HSCs and PCs to peripheral blood of the patients,intravenous and intrathecal transplantations of SCs and PCs) and different types of remote non‐contact ionizing radio and electromagnetic radiation and structural‐resonance effect. The technology is the main instrument to change the biological activity of the brain NT,to manage the brain functions,to purposefully affect cognitive functions of the brain,activate memory and reduce negative memories and emotions, and to relieve the stress and psychogenic,optimize functions of the brain and enhance intellectual potential and memory reserves.The practical goal in developing this innovative technology of remote bioengineering of the brain and/or spinal cord NT was so that it will be an alternative to the available neurosurgical,endoscopic and radio‐surgical reconstruction of the brain and spinal cord. The solution was found in the patterns of the fundamental neurobiology of the human brain, analysis of the information structure of injuries of the brain and spinal cord and in the management of the neurobiological phenomena of migration,pathtropism and regulatory properties of the SCs and PCs of humans,as well as in the use of strict algorithms in the application of the technologies of radio diagnostics and therapy: stereotaxic radiotherapy,structuralresonance therapy,effect of EHF therapy on the cell systems and use of all range of mobilization of autologous stem and progenitor cells,methodologically united by novel ideology and methodology of the remote wireless and non‐contact radio‐neuro‐restoration of the NT of the brain and spinal cord.
The technology is based on consecutive multi‐stage program combinations and uses the already approved for clinical application methods of radio‐surgical, radio therapeutic,structural‐resonance,ultrasonic regulatory multi‐wave and cellular effect on the structure and functions of the injured NT of the brain and spinal cord. The novel methodology of selective stepwise reconstruction of the NT by cell and tissueengineering technologies,stereotaxic technologies of radiotherapy,bio‐resonance and ultrasound therapy was applied in the framework of the novel concept of non‐contact and wireless neuro‐restoration and restoration of molecular‐cellular mechanisms of functioning of the injured brain. Regeneration and/or replacement of the cells of damaged NT is achieved by means of targeted plastic effect on the appropriate areas of NT of the autologous HSCs or transplanted donor haploidentical HSC,MSSCs or PCs. These basic elements of the technology allowed for new highly effective multi‐wave radio‐bioengineering method of the restoration of NT of the brain/spinal cord in different nervous and mental diseases.
Therefore,distinct from the surgical prototypes of this technology,the breakthrough in the proposed new technology is in the implementation of the methodology and surgical approach to bioengineering the NT from the brain and spinal cord through noncontact, wireless and remote multipurpose multi‐wave ionizing and non‐ionizing biophysical reconstructive techniques. Each of the aforementioned methods of ionizing and non‐ionizing electromagnetic‐wave effects with different types of radiation can be used in the clinical practice of the Russian Federation and abroad,and is widely used in the therapy of neurologic disorders as one of the methods of physiotherapy or radiotherapy. However,local application of the methods was limited to physiotherapeutic use and does not allow for the necessary clinical effects of NT reconstruction. Today these technologies are only assisting methods in the complex pharmaceutical therapy of nervous and mental diseases,and if used correctly,they can become the main tool for the restoration of the disordered structure and function of damaged NT of the brain and spinal cord. The proposed method of the remote radio‐bioengineering overcomes all the disadvantages of current minimally invasive surgical techniques and fulfills all stages of the restoration of human brain/spinal cord without direct contact with the tissue. The reconstructiverestorative effect on specific morphofunctional structure of NT was technically realized by molecular‐cellular and wave mechanisms of NT homeostasis in the site of injury of the brain/spinal cord.
Regulation of the morphological structure reconstruction in the damaged NT was achieved by means of the approved for clinical use in Russia with medical equipment for the remote multi‐wave and ionizing effects on the cells of damaged human NT (equipment for structural‐resonance therapy and for stereotaxic radiotherapy and radiosurgery,for SRT) without surgical methods to effect NT,and,namely,without direct contact by the hands or surgical instruments which will decrease of surgery induced complications. It was necessary to implement the main program algorithms of the bioengineering technology and the logic of stepwise reconstruction of the NT: (1) To bring to practice all main technological solutions of morphological and functional restoration of NT by remote bioengineering of the brain that involve different stages of the brain repair. (2) To perform super accurate computer diagnostic of all personal morphofunctional characteristics (CT,MRI,PET, MEG,EEG) of the lesion in the brain and spinal cord. (3) To provide for targeted delivery of the cells systems of SCs and PCs or native autologous tissue‐specific SCs and PCs to the site of tissue engineering. (4) To induce stimulating and reconstructive effect on the NT. (5) To change the geometry of the vascular bed of the site of injury with due respect to all our observations and available challenges of reconstruction. (6) To open and close the BBB in due time,for a due period and in due place of the brain and spinal cord. (7) To remotely synchronize somatic and vegetative components of NT in the site of reconstruction. (8) To restore the disordered function of the damaged area of the NT of the brain/spinal cord.
This technology can be highly efficient in the correction of the consequences of acute injuries of the brain. The opportunities it provides can lead to breakthroughs in the therapy of nerve diseases,neurooncological diseases as well as a range of common civilization diseases.
The novelty,scientific significance and the subjectmatter of the proposed technology consists in the development of three‐dimensional models of the disease,relying on MRI,MEG,PET/CT,EEG mapping as well as the development of new software that allows for coordination and correlation of multi‐modal diagnostic information about the structure of the brain NT. In addition,these techniques include the development of an integral plan for the reconstruction of the site of injury or to monitor of the dynamics of the NT restoration. The basis of the technology is underpinned by the principles for the stereotaxic control and manipulation of low‐dose IR that allow for purposeful changes to the inductivity and magnetization of NT and regulation of the activity of the genome,transcriptome, proteome and metabolome levels of the brain NT by IR. The proposed method of stereotaxic radio‐neuroengineering of the brain expands the opportunities to apply IR to the therapy of many nervous and mental diseases in humans,particularly in cases when other methods are ineffective.
5 Conclusions The proposed method of remote,non‐contact radioneuroengineering can be widely adopted for quick non‐pharmaceutical arrest of post‐stress (neurosis‐like, psychogenic and reactive) disorders, increase of working capacity in military personnel and civil employees engaged in rescue services in the battlefield or natural disasters. The standard modules for diagnostic and therapeutic radiation,ultrasound and electromagnetic equipment are used to develop unique, biotechnological platforms to control the complexes of stereotaxic radio‐bioengineering with a new generation of medical equipment,which will provide for more intensive and beneficial treatments of nervous and mental diseases.The developed hardware platform and system of the software for the computer‐guided radioneuroengineering techniques,based on the newly understood principles of brain functioning will be able to correct neurologic and psychiatric disorders within several days. These results that cannot be achieved with any therapy,as the average time to treat neurosis and psychogeny varies from 3 to 6 months of intensive pharmaceutical therapy in psychiatric hospitals and neurosis departments.
Acknowledgements The authors express their acknowledgement to Maria Zhukova for the translation of the manuscript to English. Conflict of interests All contributing authors have no conflict of interests.| [1] | WHO. Neurological Disorders: Public Health Challenges[Online]. http://www.who.int/mental_health/neurology/neurological_disorders_report_web.pdf (accessed April 2, 2015). |
| Click to display the text | |
| [2] | Bryukhovetskiy AS. Cytoregulatory Therapy of Glial tumors of the Brain. Cell technologies in neurooncology. Moscow, Izdatelskaya gruppa RONC, 2011. (in Russian) |
| [3] | Bryukhovetskiy AS. Implantable neuroendoprosthetic system, method of its production and method of reconstructive neurosurgical operation. Patent of the Russian Federation RU 2394593, July 20, 2010. |
| Click to display the text | |
| [4] | Bryukhovetskiy AS, Dmitriyeva TB, Chekhonin VP, Zubritskiy VF, Sharayevskiy. The bioengineering method of remodeling of the vascular system of the brain. Patent of the Russian Federation RU 2152039, June 27, 2000. |
| [5] | International Association of Neurorestoratology. Beijing Declaration of International Association of Neurorestoratology (IANR). Cell Transplant 2009, 18: 487. |
| Click to display the text | |
| [6] | Ryvkina O. Nanotechnologies. 2010. www.innovprom.ru>nejroinzheneriya-i-nanotexnologii (accessed June 1, 2015). (in Russian) |
| [7] | The Human Brain Project. A Report to the European Commission. Lausanne, Switzerland: The HBP-PS Consortium[Online]. 2012. https://www.humanbrainproject.eu/documents/10180/17648/TheHBPReport_LR.pdf/18e5747e-10af-4bec-9806-d03aead57655 (Accessed November 30, 2014). |
| Click to display the text | |
| [8] | Brain Initiative Project [Online]. http://braininitiative.nih.gov/(Accessed November 30, 2014). |
| Click to display the text | |
| [9] | DARPA. Systems-Based Neurotechnology for Emerging Therapies (SUBNETS) [Online]. https://www.fbo.gov/index?s=opportunity&mode=form&id=5180458df226b0de3b0c9ec626368542&tab=core&_cview=1 (accessed April 22, 2015). |
| Click to display the text | |
| [10] | DARPA. RAM (Restoring Active Memory) Replay[Online]. https://www.fbo.gov/index?s=opportunity&mode=form&id=8cb5225b349630c17a8befd95364c80e&tab=core&_cview=1 (Accessed April 22, 2015). |
| Click to display the text | |
| [11] | Bryukhovetskiy AS, Dmitriyeva TB, Chekhonin VP, Zubritskiy VF, Krasheninnikov ME, Shumakov VI, Sharayevskiy. The method to produce the preparation of embryonic neurons of human for cytotransfusion. Patent of the Russian Federation RU 2146932, March 27, 2000. (in Russian) |
| Click to display the text | |
| [12] | Bryukhovetskiy AS. Preparation of autologous hematopoietic stem cells, method of production, cryopreservation and application for treatment of traumatic diseases of central nervous system. Patent of Russian Federation RU 2283119, September 10, 2006. (in Russian) |
| Click to display the text | |
| [13] | Bryukhovetskiy AS, Sevastyanov VI. Universal heterogeneous collagen matrix for implantation and method of its production. Patent of Russian Federation RU 2249462, April 10, 2005. (in Russian) |
| [14] | Yamaguchi S, Kuroda S, Kobayashi H, Shichinohe H, Yano S, Hida K, Shinpo K. The effects of neuronal induction on gene expression profile in bone marrow stromal cells (BMSC)—A preliminary study using microarray analysis. Brain Res 2006, 1087 (1): 15-27. |
| Click to display the text | |
| [15] | Raisman G. Sniffing out new approaches to spinal cord repair. Nat Med 2000, 4: 382-383. |
| Click to display the text | |
| [16] | Dunnett SB, Björklund A. Prospects for new restorative and neuroprotective treatments in Parkinson's disease. Nature 1999, 399(6738): 32-39. |
| Click to display the text | |
| [17] | Presman AS. Electromagnetic Fields and Living Nature. Moscow, Russia: Nauka, 1968. (in Russian) |
| [18] | Konoplyannikov AG. The Radiobiology of Stem Cells. Moscow, Russia: Energoatomizdat, 1984. (in Russian) |
| [19] | Konoplyannikov AG. Molecular and cellular mechanisms of late radiation damages. Radiats Biol Radioekol 1997, 37(4): 621-628. (in Russian) |
| Click to display the text | |
| [20] | Cifra M, Fields JZ, Farhadi A. Electromagnetic cellular interactions. Prog Biophys Mol Biol 2011, 105(3): 223-246. |
| Click to display the text | |
| [21] | Wong CH, Van der Kogel AJ. Mechanisms of radiation injury to the central nervous system: Implications for neuroprotection. Mol Interv 2004, 4 (5): 273-284. |
| Click to display the text | |
| [22] | Rodgers BE, Holmes KM. Radio-adaptiveresponse to environmentalexposures at Chernobyl. Dose Response 2008, 6(2): 209-221. |
| Click to display the text | |
| [23] | Kuzovlev OP. The Structural Resonance Therapy in Restorative Medicine. Moscow, Russia; Exposintez. 2005. (in Russian) |
| [24] | Blinkov IL, Verighin AT, Rogov GV. The methods to affect a biological object. The Patent of Russian Federation RU 2067879, October 20, 1996. (in Russian) |
| [25] | Hill CR, Bamber JC, ter Haar GR. Physical Principles of Medical Ultrasonics, 2nd ed. Sutton, Surrey, UK: Wiley, 2004. |
| [26] | Gavrilov LR. Focused Ultrasound of High Intensity in Medicine. Moscow, Russia: FAZIS, 2013. (in Russian) |
| Click to display the text | |
| [27] | Tyler WJ. Noninvasive neuromodulation with ultrasound? A continuum mechanics hypothesis. Neuroscientist 2011, 17(1):25-36. |
| Click to display the text | |
| [28] | Hynynen K, McDannold N, Clement G, Jolesz FA, Zadicario E, Killiany R, Moore T, Rosen D. Pre-clinical testing of a phased array ultrasound system for MRI-guided noninvasive surgery of the brain-A primate study. Eur J Radiol 2006, 59(2):149-156. |
| Click to display the text | |
| [29] | Ramundo-Orlando A, Gallerano GP. Terahertz radiation effects and biological applications. Journal of Infrared, Millimeter and Terahertz Waves 2009, 30 (12): 1308-1318. |
| Click to display the text | |
| [30] | Betskiy OV, Lebedeva NN. Contemporary views on the mechanisms of action of low intensive millimeter waves on biological objects. Milimitrovye Volny Vbiologhii Imeditsine 2001, 3: 5-19. (in Russian) |
| [31] | Ignasheva LP, Soboleva EI. In Proceedings of The Conference Millimeter Waves of Non-Thermal Intensity in Medicine, Survival of lethally radiated animals in transplantations of the cryopreserved bone marrow affected by EHF. Moscow, Russia, 1991, pp 352-354. (in Russian) |
| [32] | Abrakov LV. The Basics of Stereotaxic Surgery. Leningrad, Russia: Meditsina, 1975. (in Russian) |
| [33] | Petukhov SV. Biomechanics, Bionics and Symmetry. Moscow, Russia: Nauka, 1981. (in Russian) |
| Click to display the text | |
| [34] | Bryukhovetskiy AS. The Spinal Cord Injury: Injury: Cell Technologies in Therapy and Rehabilitation. Moscow, Russia: Prakticheskaya meditsina, 2010. (in Russian) |
| Click to display the text | |
| [35] | Tupitsin NN, Yaryghin VN, Bryukhovetskiy AS, Grivtsova LY, Mentkevich GL, Dolgopolov IS, Zaytsev AI, Davydov MI. Immunophenotypic peculiarities of mobilized stem (CD34+) cells in blood from patients with severe spinal cord injury. J Biol Regul Homeost Agents 2006, 20(1-2): 36-40. |
| Click to display the text | |
| [36] | Ratushnyak AS, Zapara TA, Ryabchikova EI. Influence of Submillimeter Range Electromagnetic Radiation on Neuron Systems. In Proceedings of the Third International Symposium on Modern Problems of Laser Physics. Novosibirsk, Russia, 2000, pp 177. (in Russian) |