Why does a little mean a lot when you have nothing? A brief review of cell therapy strategies for spinal cord injury
1 Introduction
After sustaining a devastating spinal cord injury (SCI)
and becoming paralyzed,a victim’s first concern is
when he or she will again be able to stand and walk.
More often than not,such miracles do not occur,and
the individual succumbs to despair. Some science
enthusiasts claim that they can help victims to walk
again without defining exactly what type of walking
is involved (e.g.,assisted or non‐assisted). Use of the
arms to propel the trunk forward or using gravity to
lean the trunk forward followed by passive forward
swinging or sliding of the feet via momentum should
not be defined as proper walking,as all such forward
trunk movements are passive and occur largely as a
result of gravitational forces. Moreover,merely walking
is not sufficient to lead a relatively independent life.
Rather,the victim must also maintain trunk stability
and his or her hand or hands must be useful.
This article aims to discuss (1) the minimum power
required for key muscles to ensure trunk stability;
(2) the minimum power required for key muscles to
facilitate walking in a paraplegic individual; and (3)
the minimum power is required for key muscles to
ensure hand usefulness or functionality. Although
these points represent long‐standing knowledge,the
precise relevance of these issues with regard to basic
function has not been fully discussed. Therefore,a gap
in knowledge remains with regard to the translation
of neurological recovery to functional performance.
Herein,knowledge about neurological recovery and
biomechanics of the musculoskeletal system complement
each other. This is important because once
armed with knowledge about the musculoskeletal
system,neuroscientists will understand the minimum
possible and necessary achievements in neural
recovery required to stabilize the trunk and ensure
limb functionality. It might be a waste of time to
expect the achievement of unachievable targets in the
near future at our current scientific level,and thus
we might deprive patients of benefits that they can
already enjoy. Without an understanding of functional
musculoskeletal system recovery,the translation of
knowledge concerning neurological functions from the
laboratory to bedside is incomplete. Despite obvious
early sensory recovery after olfactory‐ensheathing
cell transplantation,patients always expect motor
recovery[1]. Therefore,this article focuses only on
motor functions. It is intended to fill a gap and
complete the translation of knowledge concerning
motor recovery (Figure 1).
2 Minimum requirements for musculoskeletal system functionality
2.1 Stability of the trunk
The minimum power required for key muscle functioning
should be achieved in order to stabilize the trunk.
Otherwise,spinal instability will increase the difficulty
experienced by the paraplegic in using his or her limbs
efficiently and effectively,as the center of gravity
would shift constantly in an unstable body. Severe
instability might render walking and proper use of
the upper limbs virtually impossible. The key muscle
that contributes to minimal trunk stability is the
latissimus dorsi (
Figure 2). This muscle is innervated
by spinal cord segments C6-8 but physically covers a
vast area from the arms to the pelvis (two thirds of
the back),far below the expected level of innervation
for a cervical muscle. When the lower part of the trunk
is paralyzed below the C8 level,powerful bilateral
contractions of this muscle can maintain relative
trunk stability. For this reason,the latissimus dorsi
is nicknamed the “bridge muscle”
[2, 3]. It accordingly
bridges the upper and lower parts of the body.
However,this article does not aim to provide detailed
descriptions of muscle‐strengthening exercises. In
most humans,the center of gravity of the entire body
is located immediately in front of the first or second
segment of the sacrum while in a normal upright
standing position (
Figure 3)
[4]. When both feet are
firmly on the ground,the body is stable because the
center of gravity normally falls well within the margins
of the base of support: the feet.
2.2 Walking
What is the minimum power required for key muscles
to facilitate walking in a paraplegic individual? Gait is
an extremely complex mechanism that simultaneously
ensures mobility and stability of the entire body.
However,even scientific reports of the recovery of a
paraplegic toward walking too often vaguely use the
simple words “walk” and “walking” without defining
the exact meanings. These definitions require urgent
clarification to avoid confusing readers,particularly
those without knowledge of the biomechanics of
human gait (
Figure 4) and who only read the title. In
Phases b and e in
Figure 4,the person stands on one
foot. This is known as the Stance Phase. The other leg
is bent backward to gain momentum before swinging
forward to positions c and f in
Figure 4,respectively.
This is the Swing Phase. Next,the heel of the foot that
has swung forward drops and touches the ground.
It must roll over to allow the body to move forward
together with its center of gravity. This is called the
Rollover Phase from c to d and from f to g in
Figure 4
for the other leg. The cycles of both legs end here,and
the next cycles start again from b in
Figure 4.
As seen in Figure 4,walking depends upon interchangeably
lifting and moving the legs forward. It is
different from sliding,during which both feet are
on the ground at all times. It is also different from
running,during which both feet leave the ground
during one phase of the cycle. In a normal individual,
the center of gravity of the body falls between the legs.
Hence,the body is stable. During normal walking,
as the person moves forward with the lifted leg,the
other leg must remain firm on the ground to prevent
the person from falling (right foot b and left foot e
in Figure 4). In a normal individual,powerful contractions
of the hip abductors (gluteus medius,gluteus
minimus,sartorius,and tensor fasciae latae) hold the
suspended body so that it will not fall. However,in a
paraplegic these muscles are not strong enough. The
trunk will incline from side to side interchangeably
to retain the center of gravity within the area of the
standing foot (Figure 5). If the hip could be locked in
a certain position for a split second,it would increase
the stability of one‐foot standing. This can be done
relatively easily by hyperextending the trunk (i.e.,
leaning backward). Two‐legged body stabilization also
depends on knee and ankle stability. However,stability
from the hip above is already a daunting task for a
paraplegic,and thus it seems unlikely that a severely
paraplegic individual could stabilize all three joints
(hip to ankle). However,stability can be achieved
using an ankle/knee (AK) orthosis. With one foot on
the ground,the individual can hardly keep the body
stable with the center of gravity and within the small
area of contact between the foot and ground in order
to prevent himself or herself from falling. More often
than not,the individual needs to hold a standing
frame to ensure stability. Once the lifted leg drops to
the ground,the gait cycle of one leg completes and the
next cycle begins by lifting the other leg.
The hip is the most important joint with respect to
walking. Without hip flexion,the leg cannot move
forward and walk. Knee and ankle joint motions are
not essential if the leg can be lifted at the hip. During
normal walking,a person lifts the foot by bending the
thigh at the hip and the leg at the knee (Figure 3b).
He or she then swings the leg forward,followed by
forward movement of the whole body. This process is
assisted by gravity and momentum. A person can
walk with a straight leg if the knee and ankle are
immobilized. The resulting gait somewhat simulates
that of guards during a ceremonial parade (Figure 6).The leg does not need to be lifted to its full range. A
little clearance from the ground can suffice to allow
a small step forward. Using Grade 3 muscle power
according to the British Medical Research Council
(MRC),a patient can conduct minimal walking[6]. This
increase in power from Grade 2 to 3 is crucial. It
represents the difference between non‐functional and
functional,or non‐walkers and walkers. According to
the ASIA Standards,such an important improvement
or difference is ignored against the convenience of
examination in order to avoid inter‐rater discrepancy[7].
Examination strictly requires the full range for a
movement to be qualified for any grade. Thus,this
tiny but extremely important difference between nonfunctionality
and functionality is lost.
2.3 Dexterity of the hands
Walking is not the only important factor for independent
living. With the assistance of a wheelchair,a
patient and person can move around without much
difficulty and thus lead an independent life if his
or her arms and hands are sufficiently functional.
However,if the level of injury occurs at T1 or above,
the patient will encounter difficulties with respect to
an independent life. Let us next analyze how the
functions of various parts of the upper limb contribute
to the minimum required for independent living.
Regarding functions of the upper limbs,none are
more important for survival than drinking and eating.
Certain steps are required to get drinks and food
to the mouth. (1) The person must extend his or her
arm to reach the object in front of him or her. This
movement involves the shoulder abductors and
flexors (Figure 7). Both muscles are innervated by
the C5 spinal cord segment. This alone might not be
sufficient to reach the object. (2) The individual needs
to extend his or her elbow. This motion involves elbow
extensors that are innervated by the C7 spinal cord
segment (Figure 8). (3) He or she must then graspand hold the object with sufficient power (at least
Grade 3 MRC). This is the function of wrist extensors,
which are innervated by the C6 spinal cord segment.
This function passively increases tension in the finger
flexors. These combined functions of the two groups of
muscles might provide the individual with sufficient
power to hold a light object (Figure 9a). (4) Next,he
or she must retract the object to reach his or her
mouth. Again,this is a function of the elbow flexors
innervated by the C5 spinal cord segment. However,
this does not conclude the process,as the object still
must reach the mouth and retreat from it after use.
For these purposes,forearm rotation is indispensable.
Rotation towards the body (pronation) is executed
by pronator muscles that are innervated by C5-6 and,
to a lesser extent,C8-T1 (Figure 10); rotation away
from the body is executed by supinators that are
innervated by C7.
From the above‐mentioned description,we observe
that if all muscles innervated by spinal cord segments
C5-C7 are of Grade 3 MRC,the person can reach
drinks and food and thus ensure his or her survival
relatively independently. This is the minimum or
threshold that should be achieved by cell therapy for
repair of the human central nervous system.
3 Practical considerations
3.1 Motor assessment
3.1.1 MRC or ASIA Standards?
An improvement of muscle power from Grade 2 to 3
at a certain level of the spinal cord injury makes a
difference between life and death. This calls into
question the rationale of the ASIA Standards of Motor
Examination. This examination requires a full range
of movement in a joint in order to qualify a grade of
muscle power,thus avoiding ambiguity. This advantage
has been offset by the disadvantage of ignoring delicate
or even minute changes cross the entire range of joint
motion that might make vital contributions to the
activities of daily living. Apart from the author’s own
observation,a recently reported case of olfactory
ensheathing cell transplantation reinforced the view
that the traditional British MRC standard underlines
a useful increase in muscle power from non‐functional
to functional,whereas the ASIA Standards do not
[6, 7].
The author wonders if use of the ASIA Standards
is responsible for some negative reports concerning
olfactory ensheathing cell transplantation
[8]. One might
reasonably propose that MRC should be used as a
prime standard for measuring the functional outcomes
of clinical trials of cell therapy. The ASIA Standards can
be used in parallel as a supplement. After accumulating
data from a body of clinical trials that have compared
these two methods,the resulting conclusion might
indicate that only one method is reliable.
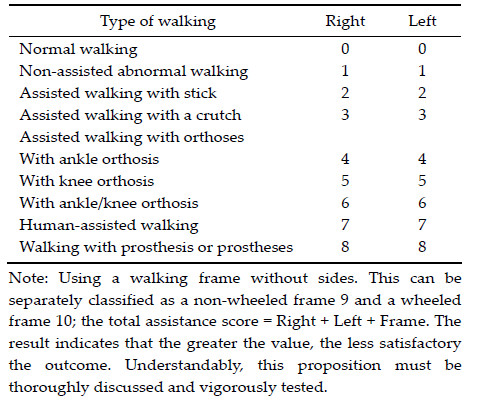
3.1.2 A modified walking grading system
Regarding walking,the motion must be classified in
more detail,rather than a general description of
walking. The author would like to propose the
following. Walking ability should be based on a test
of walking for a distance of 10 meters without falling.
This test is not intended to replace the Walking Index
for Spinal Cord Injury (WISCI Ⅱ) Descriptors developed
by Ditunnos,which are used for rehabilitation
[9, 10].
Rather,this newly proposed system is designed
specifically and solely for clinical trials of cell therapy.
Most recipients of and candidates for cell therapy
view standing and walking without human assistance
as an essential issue of image. Given this psychological
perspective,human assistance is classified as a less
satisfactory outcome in this newly proposed system.
In addition,the official terminology of orthoses based
on the extent of joint immobilization is used instead
of the word brace. This system must be tested.
3.2 Level criteria for clinical trials of cell therapy
for spinal cord injury
The author is aware of only minor improvements
in motor functions as described in a limited number
of publications from reliable sources and his own
observations for more than a decade
[11, 12, 13, 14]. For safety
reasons,clinical trials of cell transplantation prefer
treatment at the thoracic level
[15, 16]. However,the ISCoS
guidelines also acknowledge that recovery is more
likely at the cervical level
[17]. Another concern involves
ruling out spontaneous recovery in clinical trials; this
is more likely at the cervical level than at the thoracic
level. In the latter,the cord is often completely contused
in a narrow bony canal,and spontaneous recovery
rarely occurs at any stage of the natural course. Thus
far,no breakthroughs in major motor improvements
at this level have been reported. We do not yet know
when such breakthroughs might appear on the
horizon. These are definitely not around the corner,
and accordingly the journey ahead is long.
From the perspective of independent living,a
person injured below the cervical level can receive
assistance from a wheelchair,and cell therapy is
therefore less urgent. Injury at the cervical level
severely compromises independent living. Therefore,
repair at this level is a matter of relative urgency. It is
absolutely correct that the ISCoS guidelines note that
an “improvement of functional abilities,reflected in
activities of daily living will be the most meaningful
and valued outcome”[17]. Selection of the cervical cord
for a clinical trial is a very different scenario. The
cervical cord is enlarged at the most common injury
level,C4-6. The cord in this location is very bulky
when compared with the thoracic cord,and the incidence
of complete severance is low. Hence,recovery is
more likely to occur[18]. Whether recovery is structural
or functional is a different issue that requires a very
long time to resolve. A recent report described repeated
neurological examinations at intervals of at least
three months to rule out spontaneous recovery[12]. If
the results of the two examinations are the same,
further spontaneous recovery during clinical trial
would be considered unlikely. This report falls short
of the maximum period of spontaneous recovery of
30 months (more than two years) reported for work conducted
by Burns and Ditunno,as well as Waters[17, 19, 20].
Spontaneous recovery may not be a continual process.
Interval(s) might occur between episode(s) of recovery,
according to the Clinical Database,National Spinal
Injuries Centre,Stoke Mandeville Hospital. It might
therefore be more reliable to conduct clinical trials
after this maximum period to avoid the involvement of
spontaneous recovery. Currently,only limited positive
results are available after cell therapy,whereas many
patients are longing for assistance. If it is ethical to
work toward functional improvement,which might
benefit a wider population,should the SCI scientific
community rethink the strict criteria by which only
mid‐thoracic candidates are selected for clinical trials?
Table 1 A simplified scoring system for walking