摘要 Objective: The conflicting findings of previous morphological studies on intracranial aneurysm rupture may be caused by the different locations of aneurysms. We aimed to determine the independent risk factors of aneurysm rupture by focusing on only posterior communicating artery (PcomA) aneurysms. Methods: In 89 PcomA aneurysms (58 ruptured, 31 unruptured), clinical and morphological characteristics were compared between the ruptured and unruptured groups. Multivariate logistic regression analysis was performed to determine the independent predictors for the rupture status of PcomA aneurysms. Results: In univariate analyses, the aneurysm dome size, aspect ratio, size ratio, dome-to-neck ratio, and inflow angle were significant parameters. With multivariate analyses, only the aneurysm dome size and inflow angle were significantly associated with the rupture status of PcomA aneurysms. Conclusions: Morphology was related with rupture of PcomA aneurysms. The aneurysm dome size and inflow angle were found to be the independent parameters characterizing the rupture status of PcomA aneurysms.
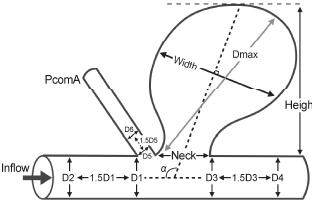
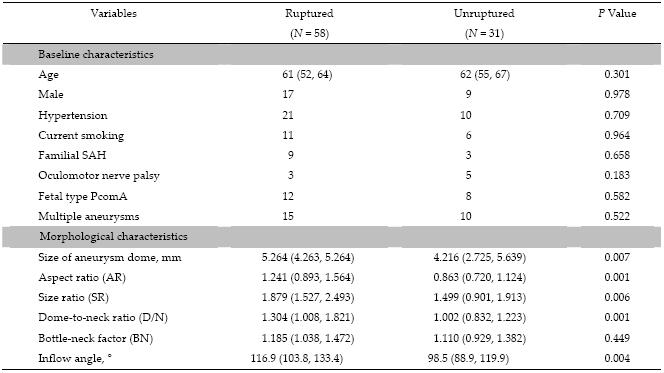
Abstract: Objective: The conflicting findings of previous morphological studies on intracranial aneurysm rupture may be caused by the different locations of aneurysms. We aimed to determine the independent risk factors of aneurysm rupture by focusing on only posterior communicating artery (PcomA) aneurysms. Methods: In 89 PcomA aneurysms (58 ruptured, 31 unruptured), clinical and morphological characteristics were compared between the ruptured and unruptured groups. Multivariate logistic regression analysis was performed to determine the independent predictors for the rupture status of PcomA aneurysms. Results: In univariate analyses, the aneurysm dome size, aspect ratio, size ratio, dome-to-neck ratio, and inflow angle were significant parameters. With multivariate analyses, only the aneurysm dome size and inflow angle were significantly associated with the rupture status of PcomA aneurysms. Conclusions: Morphology was related with rupture of PcomA aneurysms. The aneurysm dome size and inflow angle were found to be the independent parameters characterizing the rupture status of PcomA aneurysms.
[1] Korja M, Lehto H, Juvela S. Lifelong rupture risk of intracranial aneurysms depends on risk factors:A prospective Finnish cohort study. Stroke 2014, 45(7):1958-1963.
[2] Morita A, Kirino T, Hashi K, Aoki N, Fukuhara S, Hashimoto N, Takeo N, Sakai M, Teramoto A, Tominari S, Yoshimoto T. The natural course of unruptured cerebral aneurysms in a Japanese cohort. N Engl J Med 2012, 366(26):2474-2482.
[3] Bor ASE, Tiel Groenestege AT, terBrugge KG, Agid R, Velthuis BK, Rinkel GJE, Wermer MJH. Clinical, radiological, and flow-related risk factors for growth of untreated, unruptured intracranial aneurysms. Stroke 2015, 46(1):42-48.
[4] Greving JP, Wermer MJH, Brown RDJr, Morita A, Juvela S, Yonekura M, Ishibashi T, Torner JC, Nakayama T, Rinkel GJE, Algra A. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms:A pooled analysis of six prospective cohort studies. Lancet Neurol 2014, 13(1):59-66.
[5] Ujiie H, Tamano Y, Sasaki K, Hori T. Is the aspect ratio a reliable index for predicting the rupture of a saccular aneurysm? Neurosurgery 2001, 48(3):495-502.
[6] Zanaty M, Chalouhi N, Tjoumakaris SI, Fernando GL, Rosenwasser RH, Jabbour PM. Aneurysm geometry in predicting the risk of rupture. A review of the literature. Neurol Res 2014, 36(4):308-313.
[7] San Millán Ruíz D, Yilmaz H, Dehdashti AR, Alimenti A, de Tribolet N, Rüfenacht DA. The perianeurysmal environment:Influence on saccular aneurysm shape and rupture. AJNR Am J Neuroradiol 2006, 27(3):504-512.
[8] Golshani K, Ferrell A, Zomorodi A, Smith TP, Britz GW. A review of the management of posterior communicating artery aneurysms in the modern era. Surg Neurol Int 2010, 1:88.
[9] Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, Forbes GS, Thielen K, Nichols D, O'Fallon WM, Peacock J, Jaeger L, Kassell NF, Kongable Beckman GL, Torner JC; International Study of Unruptured Intracranial Aneurysms gators. Unruptured intracranial aneurysms:Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet 2003, 362(9378):103-110.
[10] Dhar S, Tremmel M, Mocco J, Kim M, Yamamoto J, Siddiqui AH, Hopkins LN, Meng H. Morphology parameters for intracranial aneurysm rupture risk assessment. Neurosurgery 2008, 63(2):185-196.
[11] Cebral JR, Mut F, Weir J, Putman C. Quantitative characterization of the hemodynamic environment in ruptured and unruptured brain aneurysms. AJNR Am J Neuroradiol 2011, 32(1):145-151.
[12] Xiang JP, Natarajan SK, Tremmel M, Ma D, Mocco J, Hopkins LN, Siddiqui AH, Levy EI, Meng H. Hemodynamicmorphologic discriminants for intracranial aneurysm rupture. Stroke 2011, 42(1):144-152.
[13] Miura Y, Ishida F, Umeda Y, Tanemura H, Suzuki H, Matsushima S, Shimosaka S, Taki W. Low wall shear stress is independently associated with the rupture status of middle cerebral artery aneurysms. Stroke 2013, 44(2):519-521.
[14] Matsukawa H, Fujii M, Akaike G, Uemura A, Takahashi O, Niimi Y, Shinoda M. Morphological and clinical risk factors for posterior communicating artery aneurysm rupture. J Neurosurg 2014, 120(1):104-110.
[15] Vlak MHM, Algra A, Brandenburg R, Rinkel GJE. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period:A systematic review and meta-analysis. Lancet Neurol 2011, 10(7):626-636.
[16] Forget TRJr, Benitez R, Veznedaroglu E, Sharan A, Mitchell W, Silva M, Rosenwasser RH. A review of size and location of ruptured intracranial aneurysms. Neurosurgery 2001, 49(6):1322-1325.
[17] Baharoglu MI, Schirmer CM, Hoit DA, Gao BL, Malek AM. Aneurysm inflow-angle as a discriminant for rupture in sidewall cerebral aneurysms:Morphometric and computational fluid dynamic analysis. Stroke 2010, 41(7):1423-1430.
[18] Tykocki T, Nauman P, Dow enko A. Morphometric predictors of posterior circulation aneurysms risk rupture. Neurol Res 2014, 36(8):733-738.
 2015, Vol. 1
2015, Vol. 1