摘要 Microvascular decompression (MVD) surgery has been popularized as an etiological treatment around the world for more than half a century. However, as a functional operation in the cerebellopontine angle, this process should be refined to enhance cure and minimize complication. After accomplishing more than 10,000 MVDs, we have learned the following concerning the operative technique: (1) the principle of MVD is to separate the neurovascular confliction, rather than isolate with prostheses; (2) identification of the conflict relies on good exposure; (3) a satisfactory working space can be created by the appropriate positioning, i.e., either a close-to-the-sigmoid craniectomy or caudorostral approach; (4) a sharp dissection of arachnoids leads to a maximal visualization of the entire intracranial course of the nerve root; (5) all vessels contacting the trigeminal nerve root should be cleared off; (6) intraoperative electrophysiological monitoring may predict the prognosis of hemifacial spasm and guide the operation; and (7) the dura must be closed with watertight stitches at the end.
Abstract: Microvascular decompression (MVD) surgery has been popularized as an etiological treatment around the world for more than half a century. However, as a functional operation in the cerebellopontine angle, this process should be refined to enhance cure and minimize complication. After accomplishing more than 10,000 MVDs, we have learned the following concerning the operative technique: (1) the principle of MVD is to separate the neurovascular confliction, rather than isolate with prostheses; (2) identification of the conflict relies on good exposure; (3) a satisfactory working space can be created by the appropriate positioning, i.e., either a close-to-the-sigmoid craniectomy or caudorostral approach; (4) a sharp dissection of arachnoids leads to a maximal visualization of the entire intracranial course of the nerve root; (5) all vessels contacting the trigeminal nerve root should be cleared off; (6) intraoperative electrophysiological monitoring may predict the prognosis of hemifacial spasm and guide the operation; and (7) the dura must be closed with watertight stitches at the end.
通讯作者:
Jun Zhong, E-mail: Dr-Zhong@139.com
E-mail: Dr-Zhong@139.com
引用本文:
Jun Zhong, Shiting Li. The ideal microvascular decompression technique should be easy and safe[J]. 临床转化神经科学, 2017, 3(1): 1-3.
Jun Zhong, Shiting Li. The ideal microvascular decompression technique should be easy and safe. Translational Neuroscience and Clinics, 2017, 3(1): 1-3.
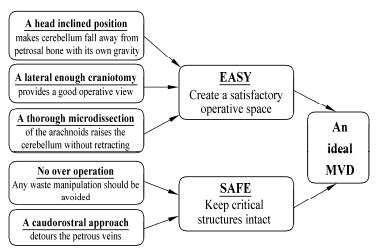
20170512094213 Figure 1 A sketch demonstrating the ideal microvascular decompression surgery (MVD) technique, which should be easy and safe.
[1]
Dou NN, Zhong J, Liu MX, Xia L, Sun H, Li B, Li ST. Teflon might be a factor accounting for a failed microvascular decompression in hemifacial spasm: A technical note. Stereotact Funct Neurosurg 2016, 94(3): 154–158.
[2]
Zhong J, Xia L, Dou NN, Ying TT, Zhu J, Liu MX, Li ST. Delayed relief of hemifacial spasm after microvascular decompression: Can it be avoided? Acta Neurochir 2015, 157(1): 93–99.
[3]
Zhong J, Zhu J, Sun H, Dou NN, Wang YN, Ying TT, Xia L, Liu MX, Tao BB, Li ST. Microvascular decompression surgery: Surgical principles and technical nuances based on 4000 cases. Neurol Res 2014, 36(10): 882–893.
[4]
Zhong J, Li ST, Zhu J, Guan HX, Zhou QM, Jiao W, Ying TT, Yang XS, Zhan WC, Hua XM. A clinical analysis on microvascular decompression surgery in a series of 3000 cases. Clin Neurol Neurosur 2012, 114(7): 846–851.
[5]
Zhu J, Zhong J, Jiao W, Zhou QM, Guan HX, Dou NN, Wang YN, Xia L, Li ST. Via-cerebellar-fissures approach for microvascular decompression of trigeminal nerve. J Craniofac Surg 2014, 25(4): 1438–1440.
[6]
Li ST, Zhong J, Sekula RF Jr. Microvascular Decompression Surgery. Netherlands: Springer, 2016.
[7]
Guan HX, Zhu J, Zhong J. Correlation between idiopathic hemifacial spasm and the MRI characteristics of the vertebral artery. J Clin Neurosci 2011, 18(4): 528–530.
[8]
Zhong J. An ideal microvascular decompression technique should be simple and safe. Neurosurg Rev 2012, 35(1): 137–140.
[9]
Zhong J, Zhu J, Li ST, Guan HX. Microvascular decompressions in patients with coexistent hemifacial spasm and trigeminal neuralgia. Neurosurgery 2011, 68(4): 916–920.
[10]
Dou NN, Hua XM, Zhong J, Li ST. A successful treatment of coexistent hemifacial spasm and trigeminal neuralgia caused by a huge cerebral arteriovenous malformation: A case report. J Craniofac Surg 2014, 25(3): 907–910.
 2017, Vol. 3
2017, Vol. 3