摘要 Few studies have investigated the factors associated with the prognosis of children with medulloblastoma. This retrospective observational study evaluated the association of molecular subtype, clinical characteristics, and pathological types with the outcomes of children with medulloblastoma. This study included 40 patients with medulloblastoma who underwent surgical resection at the Affiliated Children's Hospital of Fudan University between January 2004 and June 2014. The primary outcome was overall survival (OS). Risk factors associated with survival, disease progression, and recurrence were analyzed by univariate Cox regression analysis; the identified significant risk factors were further analyzed by Kaplan-Meier survival curves. Immunohistochemistry analysis of Yes-associated protein 1 (YAP1) and GRB2-associated protein 1 (GAB1) was used for medulloblastoma subtype identification; 20% of tumors were the WNT subtype, and 32.5% were the SHH subtype, with the remainder being non-SHH/WNT. Factors associated with OS included M stage, calcification, cerebrospinal fluid fistula, postoperative treatment (radiotherapy, chemotherapy, or both), postoperative Karnofsky Performance Scale score, and molecular subtype (P < 0.044). Patients with the WNT subtype had better survival outcomes (hazard ratio [HR] = 0.16, 95% confidence interval [CI]: 0.05–0.58). Number of symptoms, M stage, and postoperative radiotherapy were associated with disease progression (P ≤ 0.033). The risk of recurrence increased with advanced M stage (HR = 30.71; 95% CI: 3.92–240.44, P = 0.001). Patients receiving both chemotherapy and radiotherapy were less likely to have a recurrence (P = 0.040). Molecular subtyping of medulloblastoma was more predictive of survival than histopathology in patients undergoing adjuvant therapy.
Abstract: Few studies have investigated the factors associated with the prognosis of children with medulloblastoma. This retrospective observational study evaluated the association of molecular subtype, clinical characteristics, and pathological types with the outcomes of children with medulloblastoma. This study included 40 patients with medulloblastoma who underwent surgical resection at the Affiliated Children's Hospital of Fudan University between January 2004 and June 2014. The primary outcome was overall survival (OS). Risk factors associated with survival, disease progression, and recurrence were analyzed by univariate Cox regression analysis; the identified significant risk factors were further analyzed by Kaplan-Meier survival curves. Immunohistochemistry analysis of Yes-associated protein 1 (YAP1) and GRB2-associated protein 1 (GAB1) was used for medulloblastoma subtype identification; 20% of tumors were the WNT subtype, and 32.5% were the SHH subtype, with the remainder being non-SHH/WNT. Factors associated with OS included M stage, calcification, cerebrospinal fluid fistula, postoperative treatment (radiotherapy, chemotherapy, or both), postoperative Karnofsky Performance Scale score, and molecular subtype (P < 0.044). Patients with the WNT subtype had better survival outcomes (hazard ratio [HR] = 0.16, 95% confidence interval [CI]: 0.05–0.58). Number of symptoms, M stage, and postoperative radiotherapy were associated with disease progression (P ≤ 0.033). The risk of recurrence increased with advanced M stage (HR = 30.71; 95% CI: 3.92–240.44, P = 0.001). Patients receiving both chemotherapy and radiotherapy were less likely to have a recurrence (P = 0.040). Molecular subtyping of medulloblastoma was more predictive of survival than histopathology in patients undergoing adjuvant therapy.
Jianzhong Yu, We Shi, Hao Li. Factors affecting the prognosis of children with medulloblastoma: A single institution retrospective analysis of 40 cases[J]. 临床转化神经科学, 2017, 3(1): 16-27.
Jianzhong Yu, We Shi, Hao Li. Factors affecting the prognosis of children with medulloblastoma: A single institution retrospective analysis of 40 cases. Translational Neuroscience and Clinics, 2017, 3(1): 16-27.
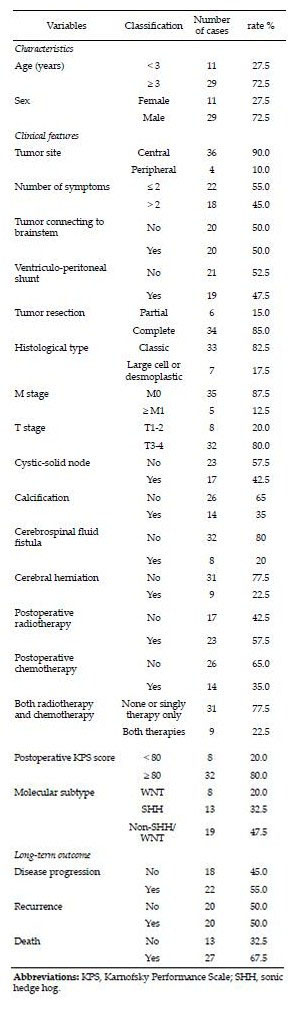
20170512093758 Table 1 Characteristics of the patients with medulloblastoma (n = 40).
20170512093838 Figure 1 Immunohistochemical analysis of YAP and GAB1 to identify medulloblastoma subtypes. (a, b) The SHH subtype was positive for both (a) YAP1 and (b) GAB1. (c, d) The WNT subtype was positive for YAP1 and negative for GAB1. (e, f) The non-SHH/WNT subtype was negative for both YAP1 and GAB1. Magnification, 400×; scale bar, 50 μm.
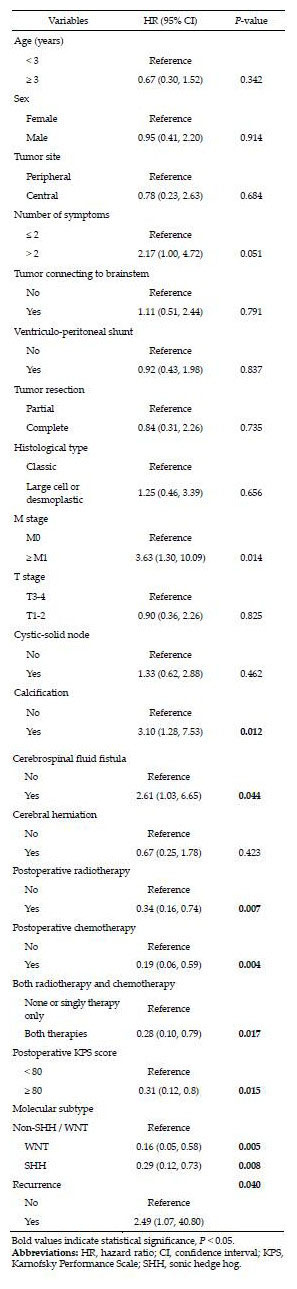
20170512093852 Table 2 Univariate Cox proportional hazard analysis of factors associated with poor survival.
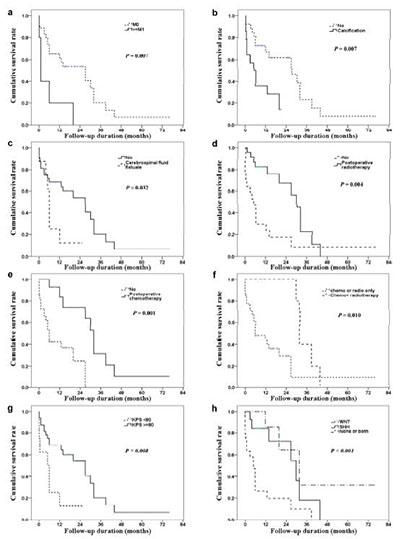
20170512093933 Figure 2 Kaplan-Meier curves of overall survival according to (a) M stage, (b) calcification, (c) cerebral fluid fistula, (d) postoperative radiotherapy, (e) postoperative chemotherapy, (f) postoperative adjuvant therapy, (g) postoperative KPS score, (h) molecular subtype. The log-rank test was used to test the survival status between groups.
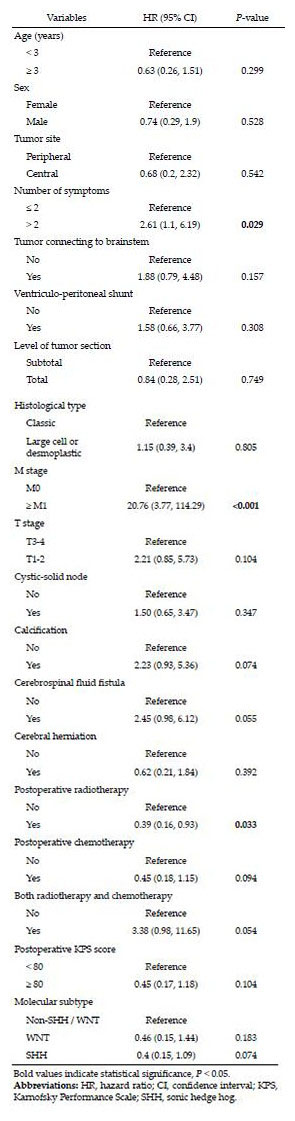
20170512093942 Table 3 Univariate Cox proportional hazard analysis of factors associated with disease progression.
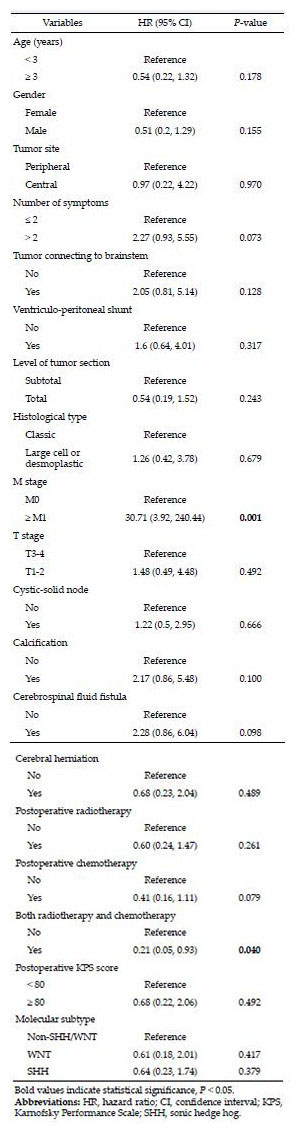
20170512093956 Table 4 Univariate Cox proportional hazard analysis of factors associated with medulloblastoma recurrence.
Gerber NU, Mynarek M, von Hoff K, Friedrich C, Resch A, Rutkowski S. Recent developments and current concepts in medulloblastoma. Cancer Treat Rev 2014, 40(3): 356-365.
[3]
Padovani L, Sunyach MP, Perol D, Mercier C, Alapetite C, Haie-Meder C, Hoffstetter S, Muracciole X, Kerr C, Wagner JP, et al. Common strategy for adult and pediatric medulloblastoma: A multicenter series of 253 adults. Int J Radiat Oncol Biol Phys 2007, 68(2): 433-440.
[4]
Rieken S, Mohr A, Habermehl D, Welzel T, Lindel K, Witt O, Kulozik AE, Wick W, Debus J, Combs SE. Outcome and prognostic factors of radiation therapy for medulloblastoma. Int J Radiat Oncol Biol Phys 2011, 81(3): e7-e13.
[5]
Pfister S, Remke M, Benner A, Mendrzyk F, Toedt G, Felsberg J, Wittmann A, Devens F, Gerber NU, Joos S, et al. Outcome prediction in pediatric medulloblastoma based on DNA copy-number aberrations of chromosomes 6q and 17q and the MYC and MYCN loci. J Clin Oncol 2009, 27(10): 1627-1636.
[6]
Pfister SM, Korshunov A, Kool M, Hasselblatt M, Eberhart C, Taylor MD. Molecular diagnostics of CNS embryonal tumors. Acta Neuropathol 2010, 120(5): 553-566.
[7]
Ellison DW, Dalton J, Kocak M, Nicholson SL, Fraga C, Neale G, Kenney AM, Brat DJ, Perry A, Yong WH, et al. Medulloblastoma: Clinicopathological correlates of SHH, WNT, and non-SHH/WNT molecular subgroups. Acta Neuropathol 2011, 121(3): 381-396.
[8]
Kool M, Korshunov A, Remke M, Jones DTW, Schlanstein M, Northcott PA, Cho YJ, Koster J, Schouten-van Meeteren A, van Vuurden D, et al. Molecular subgroups of medulloblastoma: An international meta-analysis of transcriptome, genetic aberrations, and clinical data of WNT, SHH, Group 3, and Group 4 medulloblastomas. Acta Neuropathol 2012, 123(4): 473-484.
[9]
Mamanova L, Coffey AJ, Scott CE, Kozarewa I, Turner EH, Kumar A, Howard E, Shendure J, Turner DJ. Targetenrichment strategies for next-generation sequencing. Nat Methods 2010, 7(2): 111-118.
[10]
Zhang ZY, Xu J, Ren Y, Yao Y, Li KKW, Ng HK, Mao Y, Zhou LF, Zhong P. Medulloblastoma in China: Clinicopathologic analyses of SHH, WNT, and non-SHH/WNT molecular subgroups reveal different therapeutic responses to adjuvant chemotherapy. PLoS One 2014, 9(6): e99490.
[11]
Wilson M, Gill SK, MacPherson L, English M, Arvanitis TN, Peet AC. Noninvasive detection of glutamate predicts survival in pediatric medulloblastoma. Clin Cancer Res 2014, 20(17): 4532-4539.
[12]
Pietsch T, Schmidt R, Remke M, Korshunov A, Hovestadt V, Jones DTW, Felsberg J, Kaulich K, Goschzik T, Kool M, et al. Prognostic significance of clinical, histopathological, and molecular characteristics of medulloblastomas in the prospective HIT2000 multicenter clinical trial cohort. Acta Neuropathol 2014, 128(1): 137-149.
[13]
Northcott PA, Korshunov A, Witt H, Hielscher T, Eberhart CG, Mack S, Bouffet E, Clifford SC, Hawkins CE, French P, et al. Medulloblastoma comprises four distinct molecular variants. J Clin Oncol 2011, 29(11): 1408-1414.
[14]
Kiltie AE, Lashford LS, Gattamaneni HR. Survival and late effects in medulloblastoma patients treated with craniospinal irradiation under three years old. Med Pediatr Oncol 1997, 28(5): 348-354.
[15]
Rutkowski S, von Hoff K, Emser A, Zwiener I, Pietsch T, Figarella-Branger D, Giangaspero F, Ellison DW, Garre ML, Biassoni V, et al. Survival and prognostic factors of early childhood medulloblastoma: An international meta-analysis. J Clin Oncol 2010, 28(33): 4961-4968.
[16]
Khafaga Y, Kandil AE, Jamshed A, Hassounah M, DeVol E, Gray AJ. Treatment results for 149 medulloblastoma patients from one institution. Int J Radiat Oncol Biol Phys 1996, 35(3): 501-506.
[17]
Zeltzer PM, Boyett JM, Finlay JL, Albright AL, Rorke LB, Milstein JM, Allen JC, Stevens KR, Stanley P, Li H, et al. Metastasis stage, adjuvant treatment, and residual tumor are prognostic factors for medulloblastoma in children: Conclusions from the Children's Cancer Group 921 randomized phase III study. J Clin Oncol 1999, 17(3): 832-845.
[18]
Pogorzala M, Styczynski J, Wysocki M. Survival and prognostic factors in children with brain tumors: Long-term follow-up single center study in Poland. Anticancer Res 2014, 34(1): 323-326.
[19]
Modha A, Vassilyadi M, George A, Kuehn S, Hsu E, Ventureyra ECG. Medulloblastoma in children—The Ottawa experience. Childs Nerv Syst 2000, 16(6): 341-350.
[20]
Kaur K, Kakkar A, Kumar A, Mallick S, Julka PK, Gupta D, Suri A, Suri V, Sharma MC, Sarkar C. Integrating molecular subclassification of medulloblastomas into routine clinical practice: A simplified approach. Brain Pathol 2016, 26(3): 334-343.
 2017, Vol. 3
2017, Vol. 3