Intrasellar cavernous hemangioma:A case report and literature review
Xinmin Wu1, Hongquan Yu1, Gang Zhao1, Le Wang2, Yang Liu3, Yunqian Li1
1 Department of Neurosurgery, the First Hospital of Jilin University, Changchun 130021, China;
2 Department of Ophthalmology, the First Hospital of Jilin University, Changchun 130021, China;
3 Department of Radiology, the First Hospital of Jilin University, Changchun 130021, China
Intrasellar cavernous hemangioma:A case report and literature review
Xinmin Wu1, Hongquan Yu1, Gang Zhao1, Le Wang2, Yang Liu3, Yunqian Li1
1 Department of Neurosurgery, the First Hospital of Jilin University, Changchun 130021, China;
2 Department of Ophthalmology, the First Hospital of Jilin University, Changchun 130021, China;
3 Department of Radiology, the First Hospital of Jilin University, Changchun 130021, China
摘要 Intrasellar cavernous hemangioma is rare.There are no specific symptoms and the mass effect often mimics pituitary macroadenoma.We present one case of intrasellar cavernous hemangioma that was misdiagnosed.Progressively decreasing vision was the main symptom in this case.The prolactin level was mildly increased but other biochemistry examinations were normal.Magnetic resonance imaging showed an enlarged pituitary fossa and an irregular solid tumor (33 mm×22 mm×22 mm) in the sella turcica and parasellar region.Subtotal removal in the case was performed through a transsphenoidal approach.Postoperatively,the patient's visual acuity improved.Through a literature review of 8 intrasellar cavernous hemangiomas,we found most lesions are likely to extend into the suprasellar cistern and cavernous sinus,and total resection is difficult.Transsphenoidal approach surgery should be applied for decompression of the optic nerve and biopsy,and stereotactic radiosurgery is preferable.
Abstract: Intrasellar cavernous hemangioma is rare.There are no specific symptoms and the mass effect often mimics pituitary macroadenoma.We present one case of intrasellar cavernous hemangioma that was misdiagnosed.Progressively decreasing vision was the main symptom in this case.The prolactin level was mildly increased but other biochemistry examinations were normal.Magnetic resonance imaging showed an enlarged pituitary fossa and an irregular solid tumor (33 mm×22 mm×22 mm) in the sella turcica and parasellar region.Subtotal removal in the case was performed through a transsphenoidal approach.Postoperatively,the patient's visual acuity improved.Through a literature review of 8 intrasellar cavernous hemangiomas,we found most lesions are likely to extend into the suprasellar cistern and cavernous sinus,and total resection is difficult.Transsphenoidal approach surgery should be applied for decompression of the optic nerve and biopsy,and stereotactic radiosurgery is preferable.
Xinmin Wu, Hongquan Yu, Gang Zhao, Le Wang, Yang Liu, Yunqian Li. Intrasellar cavernous hemangioma:A case report and literature review[J]. 临床转化神经科学, 2017, 3(2): 111-115.
Xinmin Wu, Hongquan Yu, Gang Zhao, Le Wang, Yang Liu, Yunqian Li. Intrasellar cavernous hemangioma:A case report and literature review. Translational Neuroscience and Clinics, 2017, 3(2): 111-115.
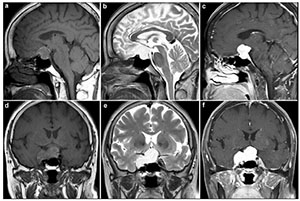
20170712150321 Figure 1 Preoperative MRI revealed a large tumor in the sella turcica. a. The tumor has marked iso-intensity on a T1-weighted image in a sagittal view. b. The tumor has marked hyperintensity on a T2-weighted image in a sagittal view. c. The tumor is brightly enhanced in a sagittal view. d. The tumor has marked iso-intensity on a T1-weighted image in a coronal view. e. The tumor shows marked hyperintensity on a T2-weighted image in a coronal view. f. The tumor is brightly enhanced in a coronal view.
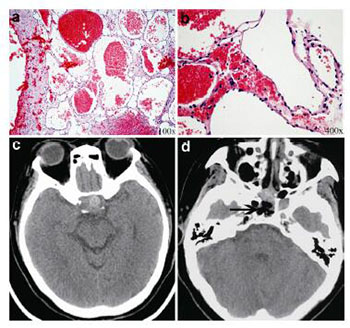
20170712150331 Figure 2 Post-operative histological and imaging examinations (a, b). On histologic examination, the mass is composed of dilated vessels occasionally containing thrombi (a, hematoxylin and eosin [H&E] stain, ×100; b, H&E stain, ×400). (c, d) Post-operative CT imaging.
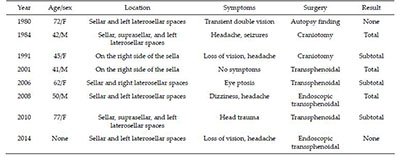
20170712150346 Table 1 Summary of the clinical profile of previously reported cases of intrasellar cavernous hemangioma[4].
[1]
Cobbs CS, Wilson CB. Intrasellar cavernous hemangioma. Case report. J. Neur. 2001, 94(3):520-522.
[2]
Lee DM, Yu SH, Yoon HH, Lee KL, Eom YS, Lee K, Kim BJ, Kim YS, Park IeB, Kim KW, Lee S. Genetic analysis of multiple endocrine neoplasia Type 1(MEN1) leads to misdiagnosis of an extremely rare presentation of intrasellar cavernous hemangioma as MEN1. End. Met. 2014, 29(2):146-153.
[3]
Ma LC, Li WY, Chen WQ, Wu YK. Intrasellar cavernous hemangioma. Neur. Ind. 2014, 62(1):95-96.
[4]
Chuang CC, Jung SM, Yang JT, Chang CN, Pai PC. Intrasellar cavernous hemangioma. J. Clini. Neur. 2006, 13(6):672-675.
[5]
Hori S, Hayashi N, Nomoto K, Sato H, Hayashi T, Nagai S, Nishikata M, Endo S. Cavernous sinus cavernous hemangioma largely extending into the sella turcica and mimicking pituitary adenoma. Neurol Med Chir (Tokyo) 2010, 50(4):330-332.
[6]
Fraser JF, Mass AY, Brown S, Anand VK, Schwartz TH. Transnasal endoscopic resection of a cavernous sinus hemangioma:Technical note and review of the literature. Skull Base 2008, 18(5):309-315.
[7]
Wang Y, Li P, Zhang XJ, Xu YY, Wang W. Gamma knife surgery for cavernous sinus hemanginoma:A report of 32 cases. World Neurosurg 2016, 94:18-25.
 2017, Vol. 3
2017, Vol. 3