Posterior mediastinal ganglioneuroma:A case report and literature review
Linkai Jing1,2, Zhenxing Sun2, Yi Guo2, Youtu Wu2, James Wang2, Guihuai Wang2
1 School of Clinical Medicine, Tsinghua University, Beijing 100084, China;
2 Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing 102218, China
Posterior mediastinal ganglioneuroma:A case report and literature review
Linkai Jing1,2, Zhenxing Sun2, Yi Guo2, Youtu Wu2, James Wang2, Guihuai Wang2
1 School of Clinical Medicine, Tsinghua University, Beijing 100084, China;
2 Department of Neurosurgery, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing 102218, China
摘要 Objectives: Ganglioneuroma is a rare,benign neurogenic tumor arising from the sympathetic ganglia.In this report,we reviewed and summarized the clinical features, treatment,and prognosis of a posterior mediastinal ganglioneuroma. Case:Here,we report on a 29-year-old man referred to us with transient pain in the right side of the chest,lasting for three days.Physical examination revealed no abnormalities. The results of routine laboratory tests were within the normal ranges.Thoracic spinal magnetic resonance imaging showed a well-defined,solid mass in the right paravertebral region at the T5-T8 level,measuring 7.5 cm×4.2 cm×1.5 cm.To accurately locate the lesion during surgery,O-arm intraoperative imaging was used in conjunction with the Stealth Station navigation system.The tumor was completely excised and no related complications occurred.The tumor was an encapsulated mass with a solid,homogenous,grayish-tan cut surface.Histopathological examinations confirmed that the mass was a ganglioneuroma. Conclusions:Ganglioneuroma is a rare,benign tumor.Prior to treatment,a careful imaging evaluation is necessary in order to obtain an accurate diagnosis.A definitive diagnosis can be made by histological examination.En bloc resection is the preferred treatment for ganglioneuroma as it has an excellent prognosis.
Abstract: Objectives: Ganglioneuroma is a rare,benign neurogenic tumor arising from the sympathetic ganglia.In this report,we reviewed and summarized the clinical features, treatment,and prognosis of a posterior mediastinal ganglioneuroma. Case:Here,we report on a 29-year-old man referred to us with transient pain in the right side of the chest,lasting for three days.Physical examination revealed no abnormalities. The results of routine laboratory tests were within the normal ranges.Thoracic spinal magnetic resonance imaging showed a well-defined,solid mass in the right paravertebral region at the T5-T8 level,measuring 7.5 cm×4.2 cm×1.5 cm.To accurately locate the lesion during surgery,O-arm intraoperative imaging was used in conjunction with the Stealth Station navigation system.The tumor was completely excised and no related complications occurred.The tumor was an encapsulated mass with a solid,homogenous,grayish-tan cut surface.Histopathological examinations confirmed that the mass was a ganglioneuroma. Conclusions:Ganglioneuroma is a rare,benign tumor.Prior to treatment,a careful imaging evaluation is necessary in order to obtain an accurate diagnosis.A definitive diagnosis can be made by histological examination.En bloc resection is the preferred treatment for ganglioneuroma as it has an excellent prognosis.
Linkai Jing, Zhenxing Sun, Yi Guo, Youtu Wu, James Wang, Guihuai Wang. Posterior mediastinal ganglioneuroma:A case report and literature review[J]. 临床转化神经科学, 2017, 3(3): 147-150.
Linkai Jing, Zhenxing Sun, Yi Guo, Youtu Wu, James Wang, Guihuai Wang. Posterior mediastinal ganglioneuroma:A case report and literature review. Translational Neuroscience and Clinics, 2017, 3(3): 147-150.
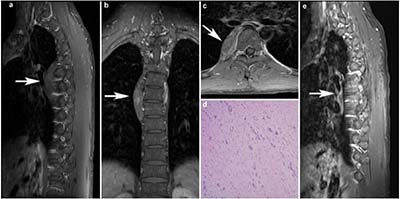
20171023160950 Figure 1 A 29-year-old male presented with transient chest pain lasting for three days. Magnetic resonance images before surgery (a, b, c) showed a solid, well-defined mass measuring 7.5 cm × 4.2 cm × 1.5 cm, in the right paravertebral region at the T5-T8 level. Histopathological examination (d) confirmed the final diagnosis of ganglioneuroma. No radiological signs of recurrence were observed seventeen months after the surgery (e).
[1]
Kumar S, Singh S, Chandna A. Organ preservation in a case of retroperitoneal ganglioneuroma:A case report and review of literature. Case Rep Surg 2016, 6597374.
[2]
Hayat J, Ahmed R, Alizai S, Awan MU. Giant ganglioneuroma of the posterior mediastinum. Interact Cardiovasc Thorac Surg 2011, 13:344-345.
[3]
Reeder LB. Neurogenic tumors of the mediastinum. Seminars in Thoracic and Cardiovascular Surgery. 2000, 12:261-267.
[4]
Przkora R, Perez-Canto A, Ertel W, Heyde CE. Ganglioneuroma:Primary tumor or maturation of a suspected neuroblastoma? Eur Spine J 2006, 15:363-365
[5]
Kizildag B, Alar T, Karatag O, Kosar S, Akman T, Cosar M. A case of posterior mediastinal ganglioneuroma:The importance of preoperative multiplanar radiological imaging. Balkan Med J 2013, 30:126-128.
[6]
Yorita K, Yonei A, Ayabe T, Nakada H, Nakashima K, Fukushima T, Kataoka H. Posterior mediastinal ganglioneuroma with peripheral replacement by white and brown adipocytes resulting in diagnostic fallacy from a false-positive 18f-2-fluoro-2-deoxyglucose-positron emission tomography finding:A case report. J Med Case Rep 2014, 8:345.
[7]
De Bernardi B, Gambini C, Haupt R, Granata C, Rizzo A, Conte M, Tonini GP, Bianchi M, Giuliano M, Luksch R, Prete A, Viscardi E, Garaventa A, Sementa AR, Bruzzi P, Angelini P. Retrospective study of childhood ganglioneuroma. J Clin Oncol 2008, 26:1710-1716.
[8]
Ozawa Y, Kobayashi S, Hara M, Shibamoto Y. Morphological differences between schwannomas and ganglioneuromas in the mediastinum:Utility of the craniocaudal length to major axis ratio. Br J Radiol 2014, 87:20130777.
[9]
Meyer S, Reinhard H, Ziegler K, Gottschling S, Aliani S, Krenn T, Graf N. Ganglianeuroma:Radiological and metabolic features in 4 children. Pediatr Hematol Oncol 2002, 19:501-508.
[10]
Paasch C, Harder A, Gatzky EJ, Ghadamgahi E, Spuler A, Siegel R. Retroperitoneal paravertebral ganglioneuroma:A multidisciplinary approach facilitates less radical surgery. World J Surg Oncol 2016, 14:194.
[11]
Retrosi G, Bishay M, Kiely EM, Sebire NJ, Anderson J, Elliott M, Drake DP, Coppi P, Eaton S, Pierro A. Morbidity after ganglioneuroma excision:Is surgery necessary? Eur J Pediatr Surg 2011, 21:33-37.
 2017, Vol. 3
2017, Vol. 3