1 Department of Neurosurgery, Changgung Hospital, Medical Center, Tsinghua University, Beijing 102218, China;
2 Department of Nephrology, Beijing Luhe Hospital, Capital Medical University, Beijing 101149, China;
3 Department of Psychiatry, Zaozhuang Mental Health Center, Zaozhuang 277103, China;
4 Department of Neurosurgery, The Fifth People's Hospital of Datong, Regional Medical Center of Shanxi Province, Datong 037006, China
Fluorescein sodium use during spinal ependymoma resection
1 Department of Neurosurgery, Changgung Hospital, Medical Center, Tsinghua University, Beijing 102218, China;
2 Department of Nephrology, Beijing Luhe Hospital, Capital Medical University, Beijing 101149, China;
3 Department of Psychiatry, Zaozhuang Mental Health Center, Zaozhuang 277103, China;
4 Department of Neurosurgery, The Fifth People's Hospital of Datong, Regional Medical Center of Shanxi Province, Datong 037006, China
摘要 Spinal ependymomas (SEs) are common adult intramedullary tumors;however, determining the absolute boundary between the tumor and the tumor residual may be difficult.We assessed outcomes following the use of fluorescein sodium (FS) during surgical removal of SEs.We performed a retrospective analysis of 112 patients with SEs who were treated at Beijing Tsinghua Changgung Hospital between December 2014 and December 2016.Each patient received intravenous FS (3-4 mg/kg) to determine the SE boundaries during surgery.Tumor removal efficiencies and tumor residuals were assessed using magnetic resonance imaging (MRI) at 10 days and 3 months after surgical recovery;McCormick's spinal function classification was also performed at the 3-month follow-up.The complete tumor removal rate was 92%(103/112).Ninetyfour patients underwent tumor removal under fluorescent light,which provided distinctive tumor fluorescence.Tumor removal under white light was performed in 18 patients;fluorescent images were invisible or indistinctive in these 18 patients.At the 3-month follow-up,sensory function (85.8%(91/106)) and movement (84.3% (86/102)) were improved in patients with pre-surgical dysfunction;urination and defecation functions were improved in 66.7%(16/24).The McCormick spinal cord functional classifications,at the 3-month follow-up,showed significant differences in the percentages of patients with disease classified to each grade (I-IV),compared with preoperative classifications (each,P<0.05).There was no MRI evidence of tumor relapse or residuals at the 3-month follow-up.FS use during the surgical treatment of SE enables complete tumor removal and detection of tumor residuals.
Abstract: Spinal ependymomas (SEs) are common adult intramedullary tumors;however, determining the absolute boundary between the tumor and the tumor residual may be difficult.We assessed outcomes following the use of fluorescein sodium (FS) during surgical removal of SEs.We performed a retrospective analysis of 112 patients with SEs who were treated at Beijing Tsinghua Changgung Hospital between December 2014 and December 2016.Each patient received intravenous FS (3-4 mg/kg) to determine the SE boundaries during surgery.Tumor removal efficiencies and tumor residuals were assessed using magnetic resonance imaging (MRI) at 10 days and 3 months after surgical recovery;McCormick's spinal function classification was also performed at the 3-month follow-up.The complete tumor removal rate was 92%(103/112).Ninetyfour patients underwent tumor removal under fluorescent light,which provided distinctive tumor fluorescence.Tumor removal under white light was performed in 18 patients;fluorescent images were invisible or indistinctive in these 18 patients.At the 3-month follow-up,sensory function (85.8%(91/106)) and movement (84.3% (86/102)) were improved in patients with pre-surgical dysfunction;urination and defecation functions were improved in 66.7%(16/24).The McCormick spinal cord functional classifications,at the 3-month follow-up,showed significant differences in the percentages of patients with disease classified to each grade (I-IV),compared with preoperative classifications (each,P<0.05).There was no MRI evidence of tumor relapse or residuals at the 3-month follow-up.FS use during the surgical treatment of SE enables complete tumor removal and detection of tumor residuals.
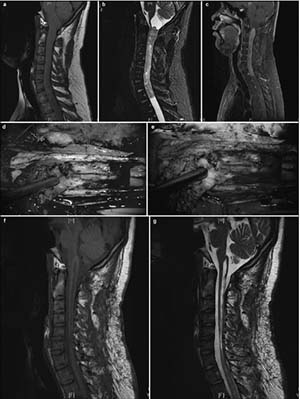
20171023161526 Figure 1 Pre- and postoperative magnetic resonance imaging of intramedullary ependymomas at C1–T1, and intraoperative observations. (a) Preoperative sagittal T1 image reveals spinal cord thickening. (b) T2 image shows high intramedullary signal intensity at C1–T1, but no signal at either end. (c) Enhanced scanning reveals distinctive tumor enhancement. (d) Intact tumor with clear boundaries, as viewed under a microscope. (e) Tumor images, viewed via fluorescence microscopy, showing a distinctive basal structure. Sagittal T1 (f) and T2 (g) images, 3 months after surgery, do not show tumor residuals or relapses.
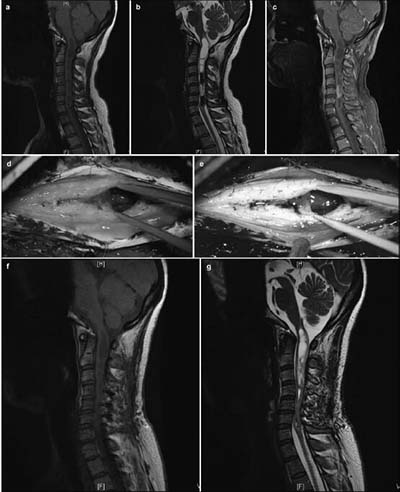
20171023161638 Figure 2 Pre- and postoperative magnetic resonance imaging of intramedullary ependymomas at C2–T2, and intraoperative observations. (a) Preoperative sagittal T1 image reveals spinal cord thickening. (b) T2 image shows high intramedullary signal intensity at C2–T2, but no signal at either end. (c) Enhanced scanning reveals distinctive enhancement of the tumor mass and cyst wall. Tumor ends, as micrographed using white light (d) and fluorescence (e). (f) Cysts at the tumor ends, microscopically probed with white light, do not show the tumor. (g) Distinct cyst walls are evident under fluorescent illumination, revealing a suspicious tumor that was removed. At 3 months, the sagittal T1 (h) and T2 (i) images and the enhanced scan (j) reveal no evidence of tumor residuals or relapses.
20171023161742 Figure 3 Intramedullary ependymomas at C3–C7, and tumor-associated stroke. (a) Preoperative T1 image showing spinal cord thickening and cysts in the septum. (b) Preoperative T2 image of a mass at C3–C7 and cysts in the septum. Stroke was not detected. (c) Preoperative enhanced magnetic resonance image showing an intramedullary tumor as a distinctive mass at C3–C7. Stroke enhancement was undetected. (d) Indistinct tumor images, intraoperatively, under fluorescent illumination. (e) Distinct intraoperative image of a tumor under the microscope. (f) Intraoperative and 1-month postoperative T1 images show the absence of tumor residuals or relapses. (g) T2 images, 1 month after surgery, show the absence of tumor residuals and relapses.
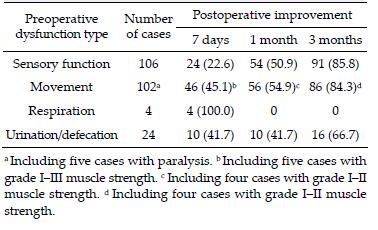
20171023161755 Table 1 Improvement in patients with spinal ependymomas demonstrating preoperative dysfunction (%).
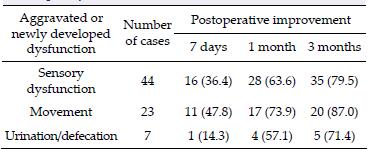
20171023161806 Table 2 Improvement in patients with aggravated or newly developed dysfunction (%).
[1]
Keil VC, Schmitt AJ, Martin SC, Cadoux-Hudson TA, Pereira EA. Optimising treatment strategies in spinal ependymoma based on 20 years of experience at a single centre. J Clin Neurosci 2016, 29:52-58.
[2]
Ewelt C, Nemes A, Senner V, Wölfer J, Brokinkel B, Stummer W, Holling M. Fluorescence in neurosurgery:its diagnostic and therapeutic use. Review of the literature. J Photochem Photobiol B 2015, 148:302-309.
[3]
Ehrhardt A, Stepp H, Irion KM, Stummer W, Zaak D, Baumgartner R, Hofstetter A. Fluorescence detection of human malignancies using incoherent light systems. Med Laser Appl 2003, 18(1):27-35.
[4]
Kukreja S, Ambekar S, Sharma M, Sin AM, Nanda A. Outcome predictors in the management of spinal myxopapillary ependymoma:an integrative survival analysis. World Neurosurg 2015, 83(5):852-859.
[5]
Xie TH, Qian Jun, Wu XJ, Lu YC, Hu GH, Luo C. Unilateral, multilevel, interlaminar fenestration in the removal of a multisegment cervical intramedullary ependymoma. Spine J 2013, 13(7):747-753.
[6]
Kim DH, Kim JH, Choi SH, Sohn Ch, Yun TJ, Kim CH, Chang KH. Differentiation between Intramedullary spinal ependymoma and astrocytoma:comparative MRI analysis. Clin Radiol 2014, 69(1):29-35.
[7]
Butte PV, Mamelak AN, Nuno M, Bannykh SI, Black KL, Marcu L. Fluorescence lifetime spectroscopy for guided therapy of brain tumors. NeuroImage 2011, 54(Suppl 1):S125-S135.
[8]
Wang GH, Yang J, Liu C, Han B, Li DZ, Chen SY, Yang B. Microneurosurgical management of intramedullary spinal cord ependymomas:report of 173 cases. Chin J Neuro-Oncol 2007, 5(1):9-12. (in Chinese)
[9]
Chen B, Wang HF, Ge PF, Zhao JW, Li WC, Gu HZ, Wang GM, Luo YA, Chen DW. Gross total resection of glioma with the intraoperative fluorescence-guidance of fluorescein sodium. Int J Med Sci 2012, 9(8):708-714.
[10]
Chen Z, Jian FZ, Wang YL, Lin F. Microneurosurgery of multisegmental intramedullary spinal cord ependymomas. Chin J Neurosurg 2006, 22(1):14-17.
[11]
Koc K, Anik I, Cabuk B, Ceylan S. Fluorescein sodiumguided surgery in glioblastoma multiforme:a prospective evaluation. Br J Neurosurg 2008, 22(1):99-103.
[12]
Okuda T, Kataoka K, Yabuuchi T, Yugami H, Kato A. Fluorescence-guided surgery of metastatic brain tumors using fluorescein sodium. J Clin Neurosci 2010, 17(1):118-121.
[13]
Shinoda J, Yano H, Yoshimura SI, Okumura A, Kaku Y, Iwama T, Sakai N. Fluorescence-guided resection of glioblastoma multiforme by using high-dose fluorescein sodium. J Neurosurg 2003, 99(3):597-603.
[14]
Schebesch KM, Proescholdt M, Höhne J, Hohenberger C, Hansen E, Riemenschneider M J, Ullrich W, Doenitz C, Schlaier J, Lange M, Brawanski A. Sodium fluorescein-guided resection under the YELLOW 560 nm surgical microscope filter in malignant brain tumor surgery-a feasibility study. Acta Neurochir 2013, 155(4):693-699.
[15]
Kremer P, Fardanesh M, Ding R, Pritsch M, Zoubaa S, Frei E. Intraoperative fluorescence staining of malignant brain tumors using 5-aminofluorescein-labeled albumin. Neurosurgery 2009, 64(3 Suppl):ons53-ons60.
[16]
Diaz RJ, Dios RR, Hattab EM, Burrell K, Rakopoulos P, Sabha N, Hawkins C, Zadeh G, Rutka JT, Cohen-Gadol AA. Study of the biodistribution of fluorescein in gliomainfiltrated mouse brain and histopathological correlation of intraoperative findings in high-grade gliomas resected under fluorescein fluorescence guidance. J Neurosurg 2015, 122(6):1360-1369.
 2017, Vol. 3
2017, Vol. 3