Surgical treatment of brainstem cavernous malformations with three basic skull base approaches and minimally invasive techniques:Observations in 20 patients
Wen Yin, Jianrong Ma, Yiwei Liao
Department of Neurosurgery, Xiangya Hospital, Central South University, Changsha 410008, China
Surgical treatment of brainstem cavernous malformations with three basic skull base approaches and minimally invasive techniques:Observations in 20 patients
Wen Yin, Jianrong Ma, Yiwei Liao
Department of Neurosurgery, Xiangya Hospital, Central South University, Changsha 410008, China
摘要 Objective: Brainstem cavernous malformation (BSCM) is extremely challenging for neurosurgeons in terms of surgical approach choices.In this article,we summarized our experience in skull base approaches of BSCM,and elucidated the advance of surgical treatments of brain stem cavernous malformation through reviewing recent relevant articles. Methods: We retrospectively reviewed 20 consecutive patients who underwent resection between May 1,2014 and April 30,2016.Only midline suboccipital,subtemporal approach and retrosigmoid approach were used in this series.The diagnoses of all patients were confirmed by radiological and histological examination. Results: All 20 patients were completely extirpated without surgical-related mortality.The mean follow-up period was 9.5 months (range,2-20 months).Of the 20 patients,80% symptomatic patients underwent surgery after first bleeding episode within 3 months,20% after two or more bleeding episodes by magnetic resonance imaging.After resection and during follow-up,75% of patients had an improvement in their modified Rankin scale (mRS) scores,whereas 10% were worse compared with their preoperative presentation;15% were unchanged. Conclusion: Appropriate basic surgical approach and minimally invasive techniques are necessary in preventing impairment of neurologic function.The three common basic skull base approaches,combined with minimally invasive techniques can handle most of BSCMs with good surgical results.
Abstract: Objective: Brainstem cavernous malformation (BSCM) is extremely challenging for neurosurgeons in terms of surgical approach choices.In this article,we summarized our experience in skull base approaches of BSCM,and elucidated the advance of surgical treatments of brain stem cavernous malformation through reviewing recent relevant articles. Methods: We retrospectively reviewed 20 consecutive patients who underwent resection between May 1,2014 and April 30,2016.Only midline suboccipital,subtemporal approach and retrosigmoid approach were used in this series.The diagnoses of all patients were confirmed by radiological and histological examination. Results: All 20 patients were completely extirpated without surgical-related mortality.The mean follow-up period was 9.5 months (range,2-20 months).Of the 20 patients,80% symptomatic patients underwent surgery after first bleeding episode within 3 months,20% after two or more bleeding episodes by magnetic resonance imaging.After resection and during follow-up,75% of patients had an improvement in their modified Rankin scale (mRS) scores,whereas 10% were worse compared with their preoperative presentation;15% were unchanged. Conclusion: Appropriate basic surgical approach and minimally invasive techniques are necessary in preventing impairment of neurologic function.The three common basic skull base approaches,combined with minimally invasive techniques can handle most of BSCMs with good surgical results.
Wen Yin, Jianrong Ma, Yiwei Liao. Surgical treatment of brainstem cavernous malformations with three basic skull base approaches and minimally invasive techniques:Observations in 20 patients[J]. 临床转化神经科学, 2017, 3(2): 74-83.
Wen Yin, Jianrong Ma, Yiwei Liao. Surgical treatment of brainstem cavernous malformations with three basic skull base approaches and minimally invasive techniques:Observations in 20 patients. Translational Neuroscience and Clinics, 2017, 3(2): 74-83.
20170712151240 Table 1 Signs and symptoms at presentation.
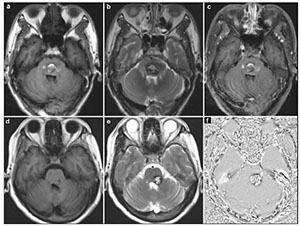
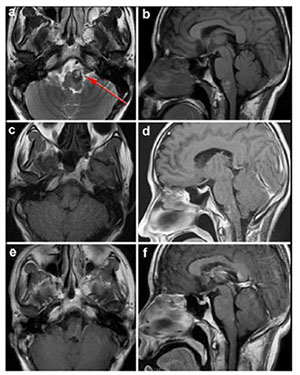
20170712151327 Figure 1 MRI demonstrated the typical “porpcorn” or “mulberry-like” BSCMs. (a), (b) and (c) showed one patient with pontine cavernoma. (d), (e) and (f) showed another patient with left cerebellar peduncle cavernoma. (a) and (d) axial T1-weighted, (b) and (e) axial T2-weighted, (c) axial enhanced T1-weighted, (f) SWI.
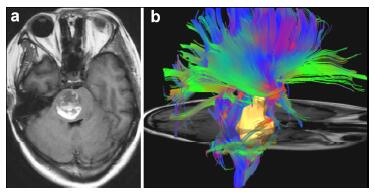
20170712151348 Figure 2 The surgical approach designed with the aid of DTI. T1-weighted (a) showed the lesion located in the right side of pontine. The three dimensional DTI (b) showed that the anterior and posterior side of the lesion was surrounded by tracts. The right approach to resect this lesion should be from the lateral side (we chose subtemporal approach).
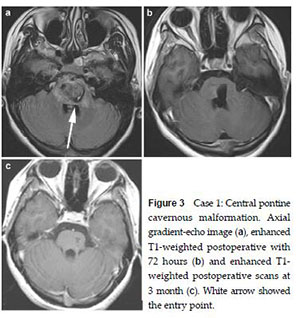
20170712151406 Figure 3 Case 1: Central pontine cavernous malformation. Axial gradient-echo image (a), enhanced T1-weighted postoperative with 72 hours (b) and enhanced T1- weighted postoperative scans at 3 month (c). White arrow showed the entry point.
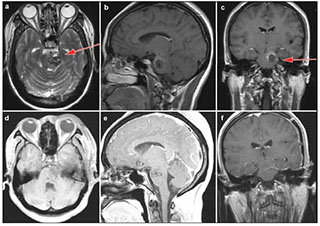
20170712151439 Figure 4 Case 2: Left anterolateral medullary cavernous malformation. Axial T2-weighted (a) and sagital T1-weighted (b) showed the location of the lesion. Axial T1-weighed (c) and enhanced sagittal T1-weighted (d) postoperative within 72 h showed that the lesion was totally resected. Enhanced axial T1-weighted (e) and enhanced sagittal T1-weighted (f) at 5-month postoperative follow-up. Red arrow showed the entry approach (retrosigmoid approach).
20170712151506 Figure 5 Case 3: Cavernous malformation in the left pons and lower midbrain. T2-weighted (a), enhanced sagittal T1-weighted (b) and enhanced coronal T1-weighted (c) demonstrated the location of the cavernous malformation. Enhanced axial T1-weighted (d) and sagittal T1-weighted (e) postoperative within 72 hours showed that the lesion was totally resected. Enhanced coronal T1-weighted (f) showed no recurrence after 3 months follow-up. Red arrow showed the entry approach (subtemporal approach).
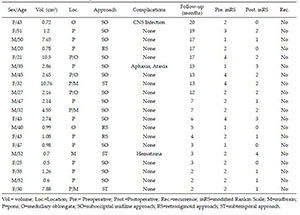
20170712151517 Table 2 Clinical characteristics of the patients with brain stem cavernous malformation.
[1]
Cantu C, Murillo-Bonilla L, Arauz A, Higuera J, Padilla J, Barinagarrementeria F. Predictive factors for intracerebral hemorrhage in patients with cavernous angiomas. Neurol Res 2005, 27(3):314-318.
[2]
Chen L, Zhao Y, Zhou L, Zhu W, Pan Z, Mao Y. Surgical strategies in treating brainstem cavernous malformations. Neurosurgery 2011, 68(3):609-620.
[3]
Gross BA, Batjer HH, Awad IA, Bendok BR, Du R. Brainstem cavernous malformations:1390 surgical cases from the literature. World Neurosurg 2013, 80(1-2):89-93.
[4]
Kim DS, Park YG, Choi JU, Chung SS, Lee KC. An analysis of the natural history of cavernous malformations. Surg Neurol 1997, 48(1):9-17.
[5]
Abla AA, Lekovic GP, Turner JD, de Oliveira JG, Porter R, Spetzler RF. Advances in the treatment and outcome of brainstem cavernous malformation surgery:A single-center case series of 300 surgically treated patients. Neurosurgery 2011, 68(2):403-414.
[6]
El Ahmadieh TY, Aoun SG, Bendok BR, Batjer HH. Management of brainstem cavernous malformations. Curr Treat Options Cardiovasc Med 2012, 14(3):237-251.
Abla AA, Spetzler RF. Brainstem cavernoma surgery:The state of the art. World Neurosurg 2013, 80(1-2):44-46.
[9]
Bogucki J, Czernicki Z, Gielecki J. Cytoarchitectonic basis for safe entry into the brainstem. Acta Neurochir (Wien) 2000, 142(4):383-387.
[10]
Kumar A, Sharma R, Garg A, Sharma BS. Contralateral anterior interhemispheric transparaterminal gyrus approach for thalamopeduncular pilocytic astrocytoma in an adult:Technical report. World Neurosurg 2016, 87:21-25.
[11]
Recalde RJ, Figueiredo EG, de Oliveira E. Microsurgical anatomy of the safe entry zones on the anterolateral brainstem related to surgical approaches to cavernous malformations. Neurosurgery 2008, 62(3 Suppl 1):9-15.
[12]
Francois P, Ben Ismail M, Hamel O, Bataille B, Jan M, Velut S. Anterior transpetrosal and subtemporal transtentorial approaches for pontine cavernomas. Acta Neurochir (Wien) 2010, 152(8):1321-1329.
[13]
Rankin J. Cerebral vascular accidents in patients over the age of 60. Ⅲ. Diagnosis and treatment. Scott Med J 1957, 2(6):254-268.
[14]
Abla AA, Lekovic GP, Garrett M, Wilson DA, Nakaji P, Bristol R, Spetzler RF. Cavernous malformations of the brainstem presenting in childhood:Surgical experience in 40 patients. Neurosurgery 2010, 67(6):1589-1598.
[15]
de Oliveira JG, Lekovic GP, Safavi-Abbasi S, Reis CV, Hanel RA, Porter RW, Preul MC, Spetzler RF. Supracerebellar infratentorial approach to cavernous malformations of the brainstem:surgical variants and clinical experience with 45 patients. Neurosurgery 2010, 66(2):389-399.
[16]
Sanborn MR, Kramarz MJ, Storm PB, Adappa ND, Palmer JN, Lee JY. Endoscopic, endonasal, transclival resection of a pontine cavernoma:case report. Neurosurgery 2012, 71(1 Suppl Operative):198-203.
[17]
Chen LH, Zhang HT, Chen L, Liu LX, Xu RX. Minimally invasive resection of brainstem cavernous malformations:Surgical approaches and clinical experiences with 38 patients. Clin Neurol Neurosurg 2014, 116:72-79.
[18]
Aiba T, Tanaka R, Koike T, Kameyama S, Takeda N, Komata T. Natural history of intracranial cavernous malformations. J Neurosurg 1995, 83(1):56-59.
[19]
Almefty KK, Spetzler RF. Management of brainstem cavernous malformations. World Neurosurg 2015, 83(3):317-319.
[20]
Chotai S, Qi S, Xu S. Prediction of outcomes for brainstem cavernous malformation. Clin Neurol Neurosurg 2013, 115(10):2117-2123.
[21]
Sekhar LN, Mantovani A. Surgical approaches to brain stem cavernous hemangiomas. World Neurosurg 2014, 82(6):1028-1029.
[22]
Mussi AC, Rhoton AL, Jr. Telovelar approach to the fourth ventricle:Microsurgical anatomy. J Neurosurg 2000, 92(5):812-823.
Steno J, Bizik I, Stenova J, Timarova G. Subtemporal transtentorial resection of cavernous malformations involving the pyramidal tract in the upper pons and mesencephalon. Acta Neurochir (Wien) 2011, 153(10):1955-1962.
[25]
Sabatino G, Rigante L, Marchese E, et al. Anterior subtemporal approach for posterolateral brainstem cavernomas:report of ten cases. Acta Neurochir (Wien) 2012, 154(11):2009-2016.
[26]
Yagmurlu K, Rhoton AL, Jr., Tanriover N, Bennett JA. Three-dimensional microsurgical anatomy and the safe entry zones of the brainstem. Neurosurgery 2014, 10(Suppl 4):602-619.
[27]
Wang CC, Liu A, Zhang JT, Sun B, Zhao YL. Surgical management of brain-stem cavernous malformations:Report of 137 cases. Surg Neurol 2003, 59(6):444-454.
[28]
Mai JC, Ramanathan D, Kim LJ, Sekhar LN. Surgical resection of cavernous malformations of the brainstem:Evolution of a minimally invasive technique. World Neurosurg 2013, 79(5-6):691-703.
[29]
Abla AA, Benet A, Lawton MT. The far lateral transpontomedullary sulcus approach to pontine cavernous malformations:Technical report and surgical results. Neurosurgery 2014,10(Suppl 3):472-480.
[30]
Yasargil MG, Reichman MV, Kubik S. Preservation of the frontotemporal branch of the facial nerve using the interfascial temporalis flap for pterional craniotomy. Technical article. J Neurosurg 1987, 67(3):463-466.
[31]
Hu P, Liang J, Bao Y, Li M, Ling F. The pterional transsylvian transtentorial approach to ventrolateral pontine cavernomas:Indications and techniques. World Neurosurg 2014, 82(6):1276-1282.
Abla AA, Spetzler RF. Minimally invasive, but not at the cost of maximally effective, in the surgical removal of brainstem cavernous malformations. World Neurosurg 2013, 79(5-6):638-640.
[34]
Linsler S, Oertel J. Endoscopic endonasal transclival resection of a brainstem cavernoma:A detailed account of our technique and comparison with the literature. World Neurosurg 2015, 84(6):2064-2071.
 2017, Vol. 3
2017, Vol. 3