Application of multimodal image fusion technology in brain tumor surgical procedure
Jiefei Li1, Yuqi Zhang1, Le He2, Huancong Zuo1
1. Department of Neurosurgery, Medical Center, Tsinghua University, Yuquan Hospital, Beijing 100084, China;
2. Center for Biomedical Imaging Research, Tsinghua University, Beijing 100084, China
Application of multimodal image fusion technology in brain tumor surgical procedure
Jiefei Li1, Yuqi Zhang1, Le He2, Huancong Zuo1
1. Department of Neurosurgery, Medical Center, Tsinghua University, Yuquan Hospital, Beijing 100084, China;
2. Center for Biomedical Imaging Research, Tsinghua University, Beijing 100084, China
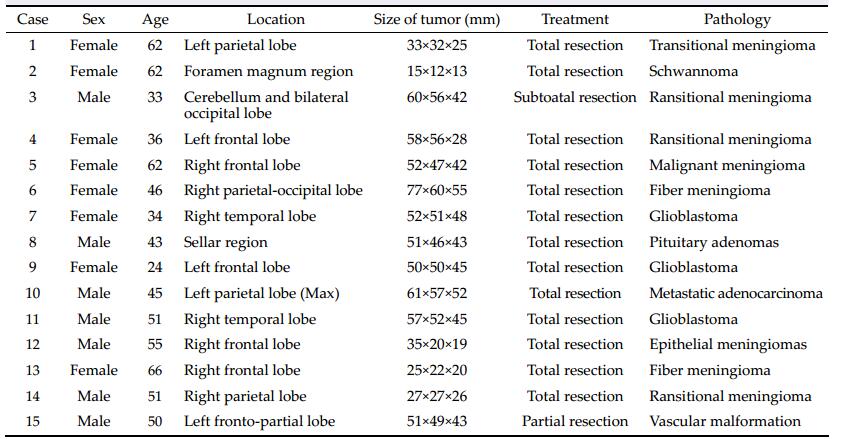
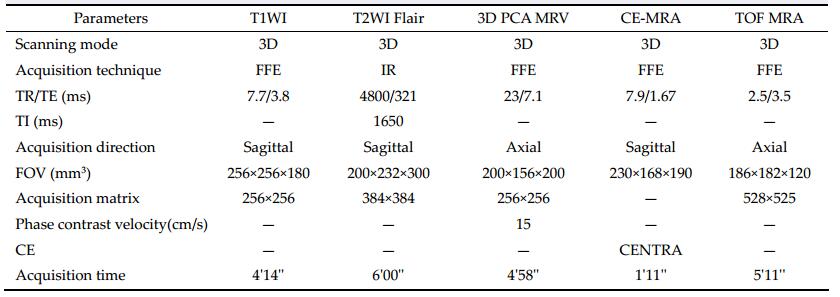
摘要 Objective: To construct brain tumors and their surrounding anatomical structures through the method of registration, fusion and, three-dimensional (3D) reconstruction based on multimodal image data and to provide the visual information of tumor, skull, brain, and vessels for preoperative evaluation, surgical planning, and function protection. Methods: The image data of computed tomography (CT) and magnetic resonance imaging (MRI) were collected from fifteen patients with confirmed brain tumors. We reconstructed brain tumors and their surrounding anatomical structures using NeuroTech software. Results: The whole 3D structures including tumor, brain surface, skull, and vessels were successfully reconstructed based on the CT and MRI images. Reconstruction image clearly shows the tumor size, location, shape, and the anatomical relationship of tumor and surrounding structures. We can hide any reconstructed images such as skull, brain tissue, blood vessles, or tumors. We also can adjust the color of reconstructed images and rotate images to observe the structures from any direction. Reconstruction of brain and skull can be semi transparent to display the deep structure; reconstruction of the structures can be axial, coronal, and sagittal cutting to show relationship among tumor and surrounding structures. The reconstructed 3D structures clearly depicted the tumor features, such as size, location, and shape, and provided visual information of the spatial relationship among its surrounding structures. Conclusions: The method of registration, fusion, and 3D reconstruction based on multimodal images to provide the visual information is feasible and practical. The reconstructed 3D structures are useful for preoperative assessment, incision design, the choice of surgical approach, tumor resection, and functional protection.
Abstract: Objective: To construct brain tumors and their surrounding anatomical structures through the method of registration, fusion and, three-dimensional (3D) reconstruction based on multimodal image data and to provide the visual information of tumor, skull, brain, and vessels for preoperative evaluation, surgical planning, and function protection. Methods: The image data of computed tomography (CT) and magnetic resonance imaging (MRI) were collected from fifteen patients with confirmed brain tumors. We reconstructed brain tumors and their surrounding anatomical structures using NeuroTech software. Results: The whole 3D structures including tumor, brain surface, skull, and vessels were successfully reconstructed based on the CT and MRI images. Reconstruction image clearly shows the tumor size, location, shape, and the anatomical relationship of tumor and surrounding structures. We can hide any reconstructed images such as skull, brain tissue, blood vessles, or tumors. We also can adjust the color of reconstructed images and rotate images to observe the structures from any direction. Reconstruction of brain and skull can be semi transparent to display the deep structure; reconstruction of the structures can be axial, coronal, and sagittal cutting to show relationship among tumor and surrounding structures. The reconstructed 3D structures clearly depicted the tumor features, such as size, location, and shape, and provided visual information of the spatial relationship among its surrounding structures. Conclusions: The method of registration, fusion, and 3D reconstruction based on multimodal images to provide the visual information is feasible and practical. The reconstructed 3D structures are useful for preoperative assessment, incision design, the choice of surgical approach, tumor resection, and functional protection.
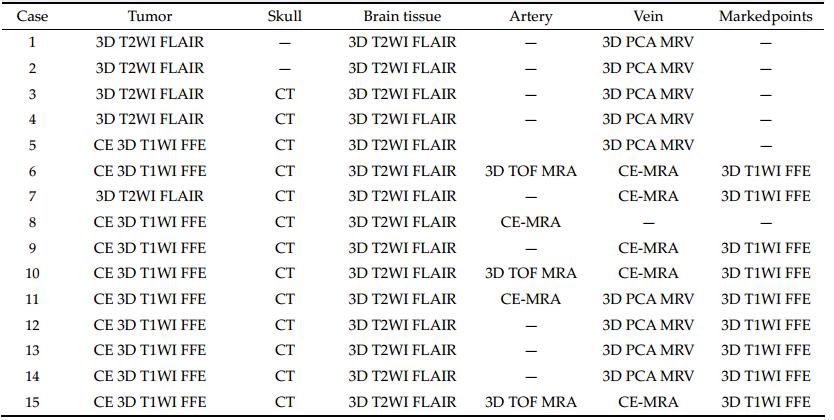
20170308095603 Table 3 Specific sources of fusion structures
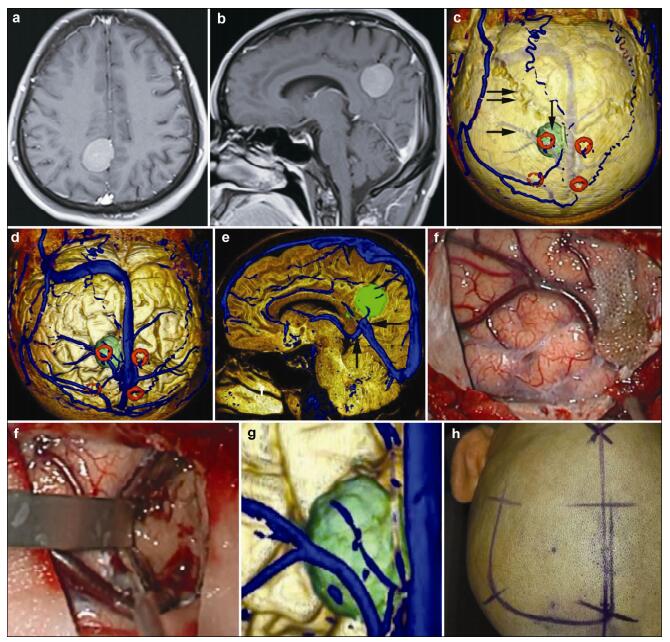
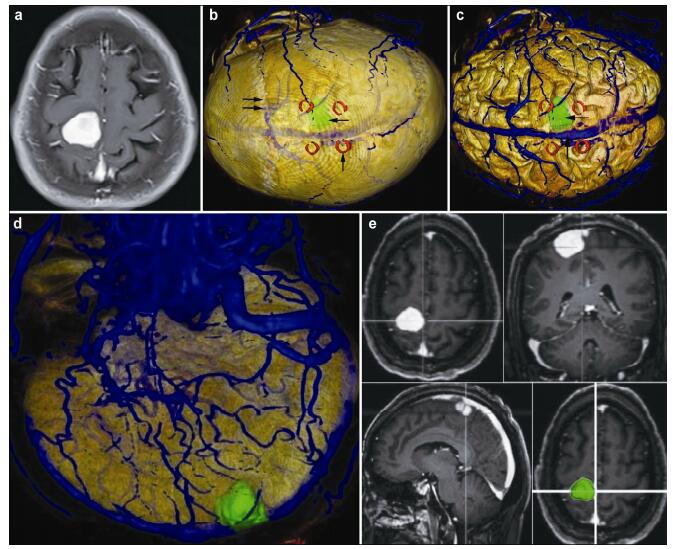
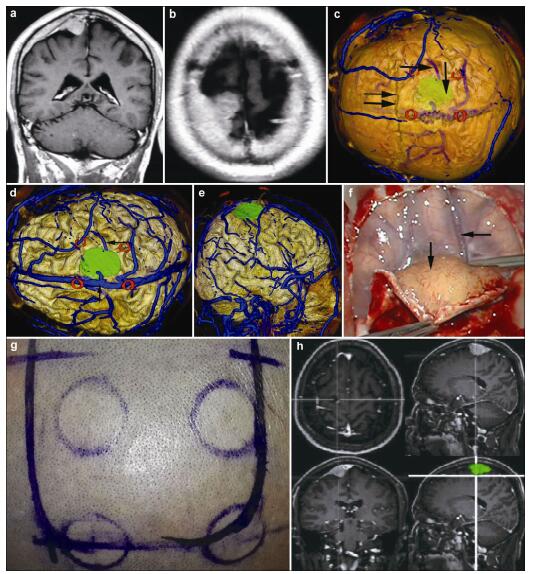
20170308095715 Figure 1 Magnetic resonance imaging, reconstruction images, surgical incision, and actual operative view in a 51-year-old male patient with a meningioma in right parietal lobe. (a, b) T1 enhancement scans: The tumor presented as homogenous enhancement. (c) 3D reconstruction (skull semitransparent): The tumor (vertical single arrow) located above lambdoidal suture (horizontal double arrow) and the superior cerebral veins (horizontal single arrow) are faintly visible. (d) 3D reconstruction (do not show the skull): On the surface of brain adjacent to the tumor are superior cerebral veins and superior sagittal sinus. (e) Sagittal cutting: The tumor is above the vein of galen and straight sinus. (f, g) The comparison of intraoperative situation and 3D reconstruction: The intraoperative situation is consistent with 3D reconstruction images. (h) Surgical incision.
20170308100004 Figure 2 Magnetic resonance imaging, reconstruction images, and 3D view of MRI in an 66-year-old female patient with a meningioma in right frontal lobe. (a) T1 enhancement scans: The tumor presented as homogenous enhancement and the precentral gyrus is located anterior to the tumor. (b) 3D reconstruction (skull semitransparent): The tumor (horizontal single arrow) located behind the coronary suture (horizontal double arrow) and the markers (vertical single arrow) are around the tumor. The superior sagittal sinus and superior cerebral veins are faintly visible. (c) 3D reconstruction (do not show the skull): The tumor (horizontal single arrow) is adjacent to the superior sagittal sinus (vertical single arrow). (d) 3D reconstruction (lateral view, brain tissue semitransparent): The tumor is adjacent to the superior sagittal sinus and locates on the surface of the brain. The positional relationship between the tumor and markers can be seen clearly. (e) 3D view: The images of 3D reconstruction are consistent with that of T1 enhancement MRI.
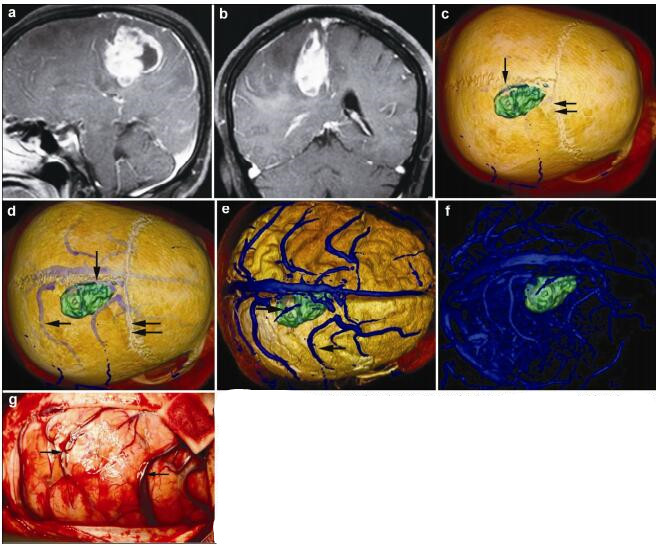
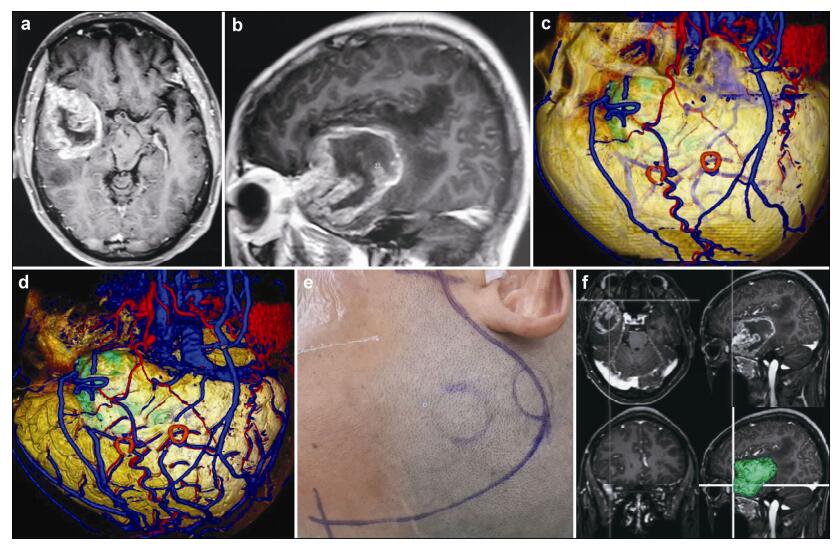
20170308100354 Figure 3 Magnetic resonance imaging, reconstruction images, and actual operative view in a 62-year-old female patient with a malignant meningioma in right frontal lobe. (a, b) T1 enhancement scans: The tumor presented as heterogeneous enhancement. (c) 3D reconstruction: The tumor located behind the coronary suture (horizontal double arrow) and adjacent to sagittal suture (vertical single arrow). (d) 3D reconstruction (skull semitransparent): This picture not only shows the relationship between tumor and sutures (coronary suture, horizontal double arrow; sagittal suture, vertical single arrow) but also shows the relationship between tumor and the superior cerebral veins (horizontal double arrow). (e) 3D reconstruction (do not show the skull): The tumor locates between two superior cerebral veins (horizontal single arrow). (f) 3D reconstruction: This picture only shows the tumor and veins. (g) Intraoperative situation: The intraoperative situation is consistent with 3D reconstruction images.
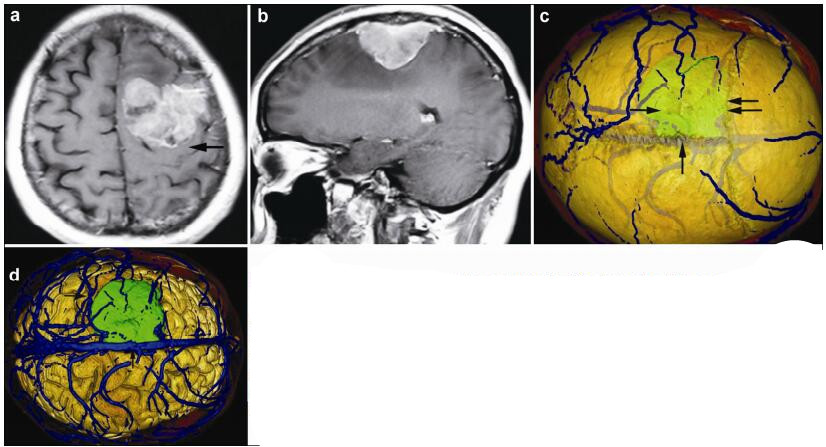
20170308100624 Figure 4 Magnetic resonance imaging and reconstruction images in a 36-year-old female patient with a meningioma in left frontal lober. (a, b) T1 enhancement scans: The tumor presented as heterogeneous enhancement and locates anerior to left postcentral gyrus (horizontal single arrow). (c) 3D reconstruction (skull semitransparent): The tumor (horizontal single arrow) located behind the coronary suture (horizontal double arrow) and adjacent to sagittal suture (vertical single arrow). (d) 3D reconstruction (do not show the skull): The tumor locates anterior to the left postcentral gyrus (vertical single arrow) and the right side of the tumor is adjacent to the superior sagittal sinus (vertical single arrow).
20170308100717 Figure 5 Magnetic resonance imaging, reconstruction images, and actual operative view in a 24-year-old female patient with a glioblastoma in left frontal lobe. (a, b) T1 enhancement scans: The tumor presented as heterogeneous enhancement. (c) 3D reconstruction: 3D reconstruction (skull semitransparent): This picture not only shows the relatioshop between tumor and sutures (vertical double arrow) but also shows the relatioshop between tumor (vertical single arrow) and the superior cerebral veins (horizontal single arrow). (d) 3D reconstruction (do not show the skull): The superior cerebral veins are shown clearly and the tumor (vertical single arrow) is under one large superior cerebral vein (horizontal single arrow). (e) 3D reconstruction (superolateral view, skull, and brian tissue semitransparent): In this picture, we can see tumor, markers, superior cerebral veins, and brain tissue simultaneously. (f) Intraoperative situation: The intraoperative situation is consistent with 3D reconstruction images.
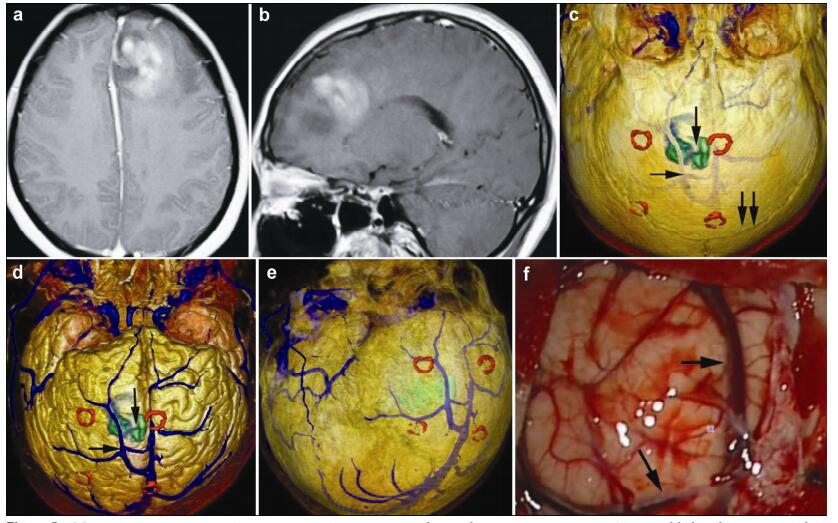
20170308100832 Figure 6 Magnetic resonance imaging, reconstruction images, surgical incision, 3D view, and actual operative view in a 55-year-old male patient with a meningioma in right frontal lobe. (a, b) T1 enhancement scans: The tumor presented as homogenous enhancement. (c) 3D reconstruction (skull semitransparent): The tumor (vertical single arrow) located behind the coronary suture (horizontal double arrow) and adjacent to sagittal suture. The right central sulcus vein (horizontal single arrow) is under the tumor. (d) 3D reconstruction (do not show the skull): The tumor is adjacent to the superior sagittal sinus (vertical single arrow) and superior sagittal sinus (vertical single arrow). (e) 3D reconstruction (lateral view): The tumor is adjacent to the superior sagittal sinus and locates on the surface of the brain above the right central sulcus vein (horizontal single arrow). The markers are around the tumor. (f) Intraoperative situation: The intraoperative situation is consistent with 3D reconstruction images. (g) Surgical incision. (h) 3D view: The images of 3D reconstruction are consistent with that of T1 enhancement MRI.
20170308100930 Figure 7 Magnetic resonance imaging, reconstruction images, surgical incision, and 3D view in a 51-year-old male patient with a glioblastoma in right frontal lobe. (a, b) T1 enhancement scans: The tumor presented as heterogeneous enhancement. (c) 3D reconstruction (skull semitransparent): The scalp blood vessels have been shown clearly. The tumor and superior cerebral veins are faintly visible. (d) 3D reconstruction (lateral view, do not show the skull): The tumor located under the markers. The veins, arteris, brian surface, and markers have shown clearly and the tumor is faintly visible. (e) Surgical incision. (f) 3D views: The images of 3D reconstruction are consistent with that of T1 enhancement MRI.
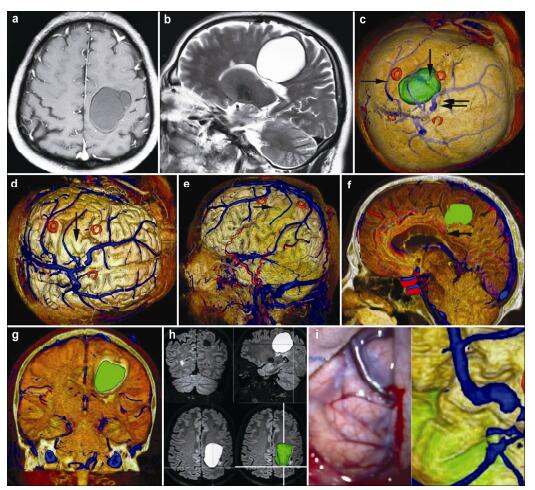
20170308101048 Figure 8 Magnetic resonance imaging, reconstruction images, surgical incision, 3D view, and actual operative view in a 51-year-old male patient with a vascular malformation in right frontal lobe. (a, b) T1 enhancement scan: The cyst presented as no enhancement; (b) T2 scan: The cyst presented as high signal. (c) 3D reconstruction (skull semitransparent): The cyst (vertical single arrow) located behind the coronary suture (horizontal double arrow) and the markers are around the cyst. The superior sagittal sinus and superior cerebral veins (horizontal single arrow) are faintly visible. (d) 3D reconstruction (do not show the skull): The cyst (vertical single arrow) is faintly visible and locates anterior to one superior cerebral vein. The veins on the surface of the brain can be seen clearly. (e) 3D reconstruction (lateral view): The cyst (horizontal single arrow) is anterior to one superior cerebral vein and locates under the motor cortex. (f) Sagittal cutting: The corpus callosum (horizontal single arrow) is compressed by the cyst. (g) Coronay cutting: The lateral ventricle and corpus callosum are compressed by the cyst. (h) 3D view: The images of 3D reconstruction are consistent with that of flair MRI. (i) The comparison of intraoperative situation and 3D reconstruction: The intraoperative situation is consistent with 3D reconstruction images.
[1]
Hosobuchi Y. Subcortical electrical stimulation for control of intractable pain in humans. J Neurosurg 1986, 64(4): 543–553.
[2]
Young RF, Kroening R, Fulton W, Feldman RA, Chambi I. Electrical stimulation of the brain in treatment of chronic pain. Experience over 5 years. J Neurosurg 1985, 62(3): 389–396.
[3]
Levy RM, Lamb S, Adams JE. Treatment of chronic pain by deep brain stimulation: Long-term follow-up and review of the literature. Neurosurgery 1987, 21(6): 885–893.
[4]
Kumar K, Toth C, Nath RK. Deep brain stimulation for intractable pain: A 15-year experience. Neurosurgery 1997, 40(4): 736–746.
Bittar RG, Kar-Purkayastha I, Owen SL, Bear RE, Green A, Wang SY, Aziz TZ. Deep brain stimulation for pain relief: A meta-analysis. J Clin Neurosci 2005, 12(5): 515–519.
[7]
Duncan GH, Kupers RC, Marchand S, Villemure JG, Gybels JM, Bushnell MC. Stimulation of human thalamus for pain relief: Possible modulatory circuits revealed by positron emission tomography. J Neurophysiol 1998, 80(6): 3326–3330.
[8]
Rezai AR, Lozano AM, Crawley AP, Joy MLG, Davis KD, Kwan CL, Dostrovsky JO, Tasker RR, Mikulis DJ. Thalamic stimulation and functional magnetic resonance imaging: localization of cortical and subcortical activation with implanted electrodes. Technical note. J Neurosurg 1999, 90(3): 583–590.
[9]
Davis KD, Taub E, Duffner F, Lozano AM, Tasker RR, Houle S, Dostrovsky JO. Activation of the anterior cingulate cortex by thalamic stimulation in patients with chronic pain: A positron emission tomography study. J Neurosurg 2000, 92(1): 64–69.
[10]
Peyron R, García-Larrea LG, Deiber MP, Cinotti L, Convers P, Sindou M, Mauguière F, Laurent B. Electrical stimulation of precentral cortical area in the treatment of central pain: Electrophysiological and PET study. Pain 1995, 62(3): 275–286.
[11]
García-Larrea LG, Peyron R, Mertens P, Gregoire MC, Lavenne F, Bonnefoi F, Mauguière F, Laurent B, Sindou M. Positron emission tomography during motor cortex stimulation for pain control. Stereotact Funct Neurosurg 1997, 68(1–4): 141–148.
[12]
Peyron R, García-Larrea LG, Grégoire MC, Convers P, Lavenne F, Veyre L, Froment JC, Mauguière F, Michel D, Laurent B. Allodynia after lateral-medullary (Wallenberg) infarct. A PET study. Brain 1998, 121(2): 345–356.
[13]
Ito M, Kuroda S, Shiga T, Tamaki N, Iwasaki Y. Motor cortex stimulation improves local cerebral glucose metabolism in the ipsilateral thalamus in patients with poststroke pain: Case report. Neurosurgery 2011, 69(2): E462–469.
[14]
Son B, Kim D, Kim H, Lee S. Simultaneous trial of deep brain and motor cortex stimulation in chronic intractable neuropathic pain. Stereotact Funct Neurosurg 2014, 92(4): 218–226.
[15]
Lévêque M, Weil AG, Nguyen JP. Simultaneous deep brain stimulation/motor cortex stimulation trial for neuropathic pain: Fishing with dynamite? Stereotact Funct Neurosurg 2015, 93: 219.
[16]
Son B, Kim MC, Moon DE, and Kang JK. Motor cortex stimulation in a patient with intractable complex regional pain syndrome type II with hemibody involvement. Case report. J Neurosurg 2003, 98(1): 175–179.
[17]
Son B. Reply to the letter by Lévêque et al. entitled ‘Simultaneous deep brain stimulation/motor cortex stimulation trial for neuropathic pain: Fishing with dynamite?’ Stereotact Funct Neurosurg 2015, 93: 220–221.
[18]
Im S, Ha S, Kim D, Son B. Long-term results of motor cortex stimulation in the treatment of chronic, intractable neuropathic pain. Stereotact Funct Neurosurg 2015, 93: 212–218.
[19]
Son B, Lee SW, Choi ES, Sung JH, Hong JT. Motor cortex stimulation for central pain following a traumatic brain injury. Pain 2006, 123(1): 210–216.
[22]
Son B, Han S, Kim D, Lee S. Motor cortex stimulation for postcordotomy dysesthetic pain. Int J Pain 2012, 3: 60–66.
[21]
Hamani C, Schwalb JM, Rezai AR, Dostrovsky JO, Davis KD, Lozano AM. Deep brain stimulation for chronic neuropathic pain: Long-term outcome and the incidence of insertional effect. Pain 2006, 125(1): 188–196.
[22]
Son B, Han SH, Choi Y, Kim M, Yang S, Lee S. Transaxillary subpectoral implantation of implantable pulse generator for deep brain stimulation. Neuromodulation 2012, 15(3): 260–266.
[23]
McCaffery M, Beebe A. Pain: Clinical Manual for Nursing Practice. London: Mosby, 1994.
[24]
Boivie J, Meyerson BA. A correlative anatomical and clinical study of pain suppression by deep brain stimulation. Pain 1982, 13(2): 113–136.
[25]
Young RF, Chambi VI. Pain relief by electrical stimulation of the periaqueductal and periventricular gray matter. Evidence for a non-opioid mechanism. J Neurosurg 1987, 66(3): 364–371.
[26]
Richardson DE, Akil H. Pain reduction by electrical brain stimulation in man. Part 1: Acute administration in periaqueductal and periventricular sites. J Neurosurg 1977, 47: 178–183.
[27]
Mazars G, Merienne L, Cioloca C. Treatment of certain types of pain with implantable thalamic stimulators. Neuro- Chirurgie 1974, 20(2): 117–124.
[28]
Pereira EAC, Boccard SG, Aziz TZ. Deep brain stimulation for pain: Distinguishing dorsolateral somesthetic and ventromedial affective targets. Neurosurgery 2014, 61: 175–181.
[29]
Fessler RG, Brown FD, Rachlin JR, Mullan S, Fang VS. Elevated beta-endorphin in cerebrospinal fluid after electrical brain stimulation: Artefact of contrast infusion? Science 1984, 224(4652): 1017–1019.
[30]
Dionne RA, Mueller GP, Young RF, Greenberg RP, Hargreaves KM, Gracely R, Dubner R. Contrast medium causes the apparent increase in β-endorphin levels in human cerebrospinal fluid following brain stimulation. Pain 1984, 20(4): 313–321.
[31]
Head J, Holmes G. Sensory disturbances from cerebral lesions. Brain 1911, 34(2–3): 102–254.
[32]
Melzack R, Wall PD. Pain mechanisms: A new theory. Science 1965, 150(3699): 971–979.
[33]
Gerhart KD, Yezierski RP, Fang ZR, Willis WD. Inhibition of primate spinothalamic tract neurons by stimulation in ventral posterior lateral (VPLc) thalamic nucleus: Possible mechanisms. J Neurophysiol 1983, 49(2): 406–423.
[34]
Benabid AL, Henriksen SJ, McGinty JF, Bloom FE. Thalamic nucleus ventro-postero-lateralis inhibits nucleus parafascicularis response to noxious stimuli through a non-opioid pathway. Brain Res 1983, 280(2): 217–231.
[35]
García-Larrea L, Peyron R, Mertens P, Laurent B, Mauguière F, Sindou M. Functional imaging and neurophysiological assessment of spinal and brain therapeutic modulation in humans. Arch Med Res 2000, 31(3): 248–257.
[36]
Maarrawi J, Peyron R, Mertens P, Costes N, Magnin M, Sindou M, Laurent B, García-Larrea L. Motor cortex stimulation for pain control induces changes in the endogenous opioid system. Neurology 2007, 69(9): 827–834.
[37]
Maarrawi J, Peyron R, Mertens P, Costes N, Magnin M, Sindou M, Laurent B, García-Larrea L. Brain opioid receptor density predicts motor cortex stimulation efficacy for chronic pain. Pain 2013, 154(11): 2563–2568.
[38]
Peyron R, Faillenot I, Mertens P, Laurent B, García-Larrea L. Motor cortex stimulation in neuropathic pain. Correlations between analgesic effect and hemodynamic changes in the brain. A PET study. Neuroimage 2007, 34(1), 310–321.
[39]
Nguyen JP, Nizard J, Keravel Y, Lefaucheur JP. Invasive brain stimulation for the treatment of neuropathic pain. Nat Rev Neurol 2011, 7: 699–709.
[40]
Raslan AM. Deep brain stimulation for chronic pain: Can it help? Pain 2006, 120(1–2): 1–2.
[41]
Plow EB, Pascual-Leone A, Machado A. Brain stimulation in the treatment of chronic neuropathic and non-cancerous pain. J Pain 2012, 13(5): 411–424.
[42]
Machado AG, Mogilner AY, Rezai AR. Motor cortex stimulation for persistent non-cancer pain. In Textbook of Stereotactic and Functional Neurosurgery. Lozano AM, Gildenberg PL, Tasker RR, Eds. Berlin Heidelberg: Springer, 2009, pp 2239–2249.
[43]
Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T, Koyama S. Chronic motor cortex stimulation in patients with thalamic pain. J Neurosurg 1993, 78(3): 393–401.
[44]
Tsubokawa T, Katayama Y, Yamamoto T, Hirayama T, Koyama S. Chronic motor cortex stimulation for the treatment of central pain. In Advances in Stereotactic and Functional Neurosurgery 9. Hitchcock ER, Broggi G, Burzaco J, Martin-Rodriguez J, Meyerson BA, Tóth S, Eds. Vienna: Springer, 1991, pp 137–139.
[45]
Tsubokawa T., Katayama Y, Yamamoto T, Hirayama T, Koyama S. Treatment of thalamic pain by chronic motor cortex stimulation. Pacing Clin Electrophysiol 1991, 14(1): 131–134.
[46]
Meyerson BA, Lindblom U, Linderoth B, Lind G, Herregodts P. Motor cortex stimulation as treatment of trigeminal neuropathic pain. In Advances in Stereotactic and Functional Neurosurgery 10. Meyerson BA, Broggi G, Martin-Rodriguez J, Ostertag C, Sindou M, Eds. Vienna: Springer, 1993, pp 150–153.
[47]
Nguyen JP, Keravel Y, Feve A, Uchiyama T, Cesaro P, Le Guerinel C, and Pollin B. Treatment of deafferentation pain by chronic stimulation of the motor cortex: report of a series of 20 cases. Acta Neurochir Suppl 1997, 68: 54–60.
[48]
Saitoh Y, Shibata M, Hirano S, Hirata M, Mashimo T, Yoshimine T. Motor cortex stimulation for central pain and peripheral deafferentation pain. Report of eight cases. J Neurosurg 2000, 92(1): 150–155.
[49]
Nguyen JP, Velasco F, Brugières P, Velasco M, Keravel Y, Boleaga B, Brito F, Lefaucheur JP. Treatment of chronic neuropathic pain by motor cortex stimulation: Results of a bicentric controlled crossover trial. Brain Stimul 2008, 1(2): 89–96.
[50]
Velasco F, Argüelles C, Carrillo-Ruiz JD, Castro G, Velasco AL, Jiménez F, Velasco M. Efficacy of motor cortex stimulation in the treatment of neuropathic pain: A randomized double-blind trial. J Neurosurg 2008, 108(4): 698–706.
[51]
Lefaucheur JP, Drouot X, Cunin P, Bruckert R, Lepetit H, Créange A, Wolkenstein P, Maison P, Keravel Y, Nguyen JP. Motor cortex stimulation for the treatment of refractory peripheral neuropathic pain. Brain 2009, 132(6): 463–1471.
[52]
Raslan AM, Nasseri M, Bahgat D, Abdu E, Burchiel KJ. Motor cortex stimulation for trigeminal neuropathic or deafferentation pain: An institutional case series experience. Stereotact Funct Neurosurg 2011, 89(2): 83–88.
[53]
Rasche D, Rinaldi PC, Young RF, Tronnier VM. Deep brain stimulation for the treatment of various chronic pain syndromes. Neurosurg Focus 2006, 21(6): E1–8.
[54]
Velasco F, Carrillo-Ruiz JD, Castro G, Argüelles C, Velasco AL, Kassian A, Guevara U. Motor cortex electrical stimulation applied to patients with complex regional pain syndrome. Pain 2009, 147(1): 91–98.
[55]
Fonoff ET, Hamani C, de Andrade DC, Yeng LT, Marcolin MA, Teixeira MJ. Pain relief and functional recovery in patients with complex regional pain syndrome after motor cortex stimulation. Stereotact Funct Neurosurg 2011, 89(3): 167–172.
[56]
Nandi D, Smith H, Owen S, Joint C, Stein J, Aziz T. Peri-ventricular grey stimulation versus motor cortex stimulation for post stroke neuropathic pain. J Clin Neurosci 2002, 9(5): 557–561.
[57]
Owen SLF, Green AL, Nandi D, Bittar RG, Wang SY, Aziz TZ. Deep brain stimulation for neuropathic pain. Neuromodulation 2006, 9(2): 100–106.
[58]
Fontaine D, Hamani C, Lozano A. Efficacy and safety of motor cortex stimulation for chronic neuropathic pain: Critical review of the literature. J Neurosurg 2009, 110(2): 251–256.
[59]
Coffey RJ, Lozano AM. Neurostimulation for chronic noncancer pain: An evaluation of the clinical evidence and recommendations for future trial designs. J Neurosurg 2006, 105(2): 175–189.
[60]
Lefaucheur JP, Ménard-Lefaucheur I, Goukon C, Keravel Y, Nguyen JP. Predictive value of rTMS in the identification of responders to epidural motor cortex stimulation therapy for pain. J Pain 2011, 12(10): 1102–1111.
[61]
Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, Haythornthwaite JA, Jensen MP, Kerns RD, Ader DN, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain 2008, 9(2): 105–121.
[62]
Geurts JW, Smits H, Kemler MA, Brunner F, Kessels AGH, van Kleef M. Spinal cord stimulation for complex regional pain syndrome type I: A prospective cohort study with longterm follow-up. Neuromodulation 2013, 16(6): 523–529.
[63]
Sears NC, Machado AG, Nagel SJ, Deogaonkar M, Stanton- Hicks M, Rezai AR, Henderson JM. Long-term outcomes of spinal cord stimulation with paddle leads in the treatment of complex regional pain syndrome and failed back surgery syndrome. Neuromodulation 2011, 14(4): 312–318.
[64]
Forouzanfar T, Weber WEJ, Kemler M, van Kleef M. What is a meaningful pain reduction in patients with complex regional pain syndrome type 1? Clin J Pain 2003, 19(5): 81–285.
[65]
Nuti C, Peyron R, Garcia-Larrea L, Brunon J, Laurent B, Sindou M, Mertens P. Motor cortex stimulation for refractory neuropathic pain: Fur year outcome and predictors of efficacy. Pain 2005, 118(1): 43–52.
[66]
Boccard SGJ, Pereira EAC, Moir L, Aziz TZ, Green AL. Long-term outcomes of deep brain stimulation for neuropathic pain. Neurosurgery 2013, 72(2): 221–231.
[67]
Kemler MA, Barendese GAM, van Kleef M, de Vet HCW, Rijks CPM, Furnée CA, van den Wildenberg FAJM. Spinal cord stimulation in patients with chronic reflex sympathetic dystrophy. N Eng J Med 2000, 343(9): 618–624.
[68]
Turner KA, Loeser JD, Deyo RA, Sanders SB. Spinal cord stimulation for patients with failed back surgery syndrome or complex regional pain syndrome: A systematic review of effectivenss and complications. Pain 2004, 108(2): 137–147.
[69]
Kemler MA, de Vet HCW, Barendse GAM, van den Wildenberg FAJM, van Kleef M. Effect of spinal cord stimulation for chronic complex regional pain syndrome Type I: Five-year final follow-up of patients in a randomized controlled trial. J Neurosurg 2008, 108(2): 292–298.
[70]
de Mos M, Huyen FJPM, van den Hoeven-Borgman M, Dieleman JP, Ch Stricker BH, Sturkenboom MCJM. Outcome of the complex regional pain syndrome. Clin J Pain 2009, 25(7): 590–597.
 2016, Vol. 2
2016, Vol. 2