1 Department of Neurosurgery, Changgung Hospital, Medical Center, Tsinghua University, Beijing 102218, China;
2 Department of Nephrology, Beijing Luhe Hospital, Capital Medical University, Beijing 101149, China;
3 Department of Psychiatry, Zaozhuang Mental Health Center, Zaozhuang 277103, China;
4 Department of Neurosurgery, The Fifth People's Hospital of Datong, Regional Medical Center Of Shanxi Province, Datong 037006, China
Application of intraoperative O-arm-assisted real-time navigation technique for spinal fixation
1 Department of Neurosurgery, Changgung Hospital, Medical Center, Tsinghua University, Beijing 102218, China;
2 Department of Nephrology, Beijing Luhe Hospital, Capital Medical University, Beijing 101149, China;
3 Department of Psychiatry, Zaozhuang Mental Health Center, Zaozhuang 277103, China;
4 Department of Neurosurgery, The Fifth People's Hospital of Datong, Regional Medical Center Of Shanxi Province, Datong 037006, China
摘要 This study explored the combined use of the O-arm and real-time navigation during spinal fixation. The clinical data for 60 patients undergoing spinal fixation, at Beijing Tsinghua Chang Gung Hospital between May 5, 2015 and May 1, 2017, were retrospectively analyzed. Pre-, intra-, and postoperative imaging findings were assessed. The patients were classified into the occipitocervical fusion (32 cases) and thoracic/lumbar/sacral spine fixation (28 cases, including 6 cases of percutaneous pedicle screw) groups. Lesion resections were performed microscopically. An O-arm, combined with real-time navigation, was used to assess spinal fixation. Efficacy was evaluated using operative times, X-ray times, screw positioning, and complications. Within the occipitocervical fusion group, 182 screws were placed in the cervical spine and 96 in the occipital bone. However, 6 screws penetrated the bone cortex and were adjacent to the vertebral arteries, based on O-arm three-dimensional imaging; therefore, the precision rate was 96.7%. Within the thoracic/lumbar/sacral spine fixation group, 148 pedicle screws were implanted, with 4 initially outside the vertebral body, yielding a precision rate of 97.3%. Ten percutaneous pedicle screws were implanted and well positioned. O-arm scans were performed 3 times/patient, with an average of 20-30 min/time. Screw implantation times were 5-7 min (cervical spine), 8-10 min (thoracic spine), and 6-8 min (lumbar spine). Intraoperative O-arm scans, combined with real-time navigation technology, allow real-time observation of screw angles and depths, improving the accuracy and safety of posterior screw fixations and reducing the radiation dose and frequency experienced by patients and surgeons.
Abstract: This study explored the combined use of the O-arm and real-time navigation during spinal fixation. The clinical data for 60 patients undergoing spinal fixation, at Beijing Tsinghua Chang Gung Hospital between May 5, 2015 and May 1, 2017, were retrospectively analyzed. Pre-, intra-, and postoperative imaging findings were assessed. The patients were classified into the occipitocervical fusion (32 cases) and thoracic/lumbar/sacral spine fixation (28 cases, including 6 cases of percutaneous pedicle screw) groups. Lesion resections were performed microscopically. An O-arm, combined with real-time navigation, was used to assess spinal fixation. Efficacy was evaluated using operative times, X-ray times, screw positioning, and complications. Within the occipitocervical fusion group, 182 screws were placed in the cervical spine and 96 in the occipital bone. However, 6 screws penetrated the bone cortex and were adjacent to the vertebral arteries, based on O-arm three-dimensional imaging; therefore, the precision rate was 96.7%. Within the thoracic/lumbar/sacral spine fixation group, 148 pedicle screws were implanted, with 4 initially outside the vertebral body, yielding a precision rate of 97.3%. Ten percutaneous pedicle screws were implanted and well positioned. O-arm scans were performed 3 times/patient, with an average of 20-30 min/time. Screw implantation times were 5-7 min (cervical spine), 8-10 min (thoracic spine), and 6-8 min (lumbar spine). Intraoperative O-arm scans, combined with real-time navigation technology, allow real-time observation of screw angles and depths, improving the accuracy and safety of posterior screw fixations and reducing the radiation dose and frequency experienced by patients and surgeons.
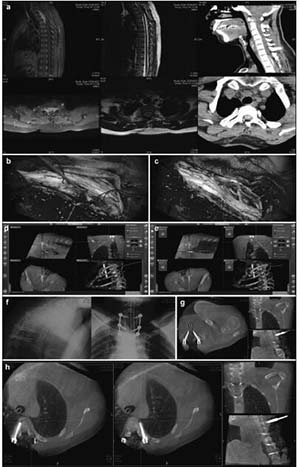
20171023161042 Figure 1 Preoperative, intraoperative, and postoperative images of patients with atlantoaxial dislocation and occipitocervical fusion. Preoperative cervical radiography in the side (a), anteflexion (b), and supine (c) positions reveals odontoid instability and a backward and upward shift. Preoperative computed tomography (CT) (d) and magnetic resonance imaging (MRI) (e) show that the backward and upward dislocation of the C2 odontoid impacts the brain stem. The foramen magnum is narrow, and the cervical cord void is visible. (f) Implantation direction and C2 angle. Pars screws are planed under intraoperative navigation. (g) O-arm three-dimensional scan, after screw implantation, shows that the Pars screw to the right of C2 penetrates the bone cortex and is near the vertebral artery. Lateral radiography (h), sagittal CT (i), and a T2 sagittal scan (j), 1 week after the operation, show firm screw fixation in a good position and inferoanterior displacement of the odontoid to the C1 level, essentially achieving normal anatomical reduction. Brain stem compression is released, and the posterior cranial fossa is fully decompressed.
20171023161255 Figure 2 Preoperative, intraoperative, and postoperative images of patients in the thoracic intraspinal meningioma resection and pedicle screw fixation group. (a) Cervical thoracic vertebrae computed tomography shows a high-density tumor shadow in the thoracic spinal canal (T1-T4). Magnetic resonance imaging shows T2 image isointensity in the spinal canal (T1-T4). An enhanced scan shows a significantly enhanced area located in the ventral spinal cord that has invaded the intervertebral foramen. (b) Intraoperative microscopy shows a spinal cord ventral tumor, originating in the dura mater. (c) Intraoperative microscopy shows nearly total resection of the spinal cord ventral tumor, with the spinal cord remaining intact. (d, e) Intraoperative T2 pedicle screw implantation is performed under real-time navigation. The entry direction, angle, and depth of the screw is according to the navigation plan. (f, g, h) After screw implantation, an O-arm two-dimensional lateral scan shows good screw positioning. The O-arm three-dimensional scan found that the T1 bilateral pedicle screws are well positioned and do not penetrate the bone cortex. The T4 left pedicle screw position is also good. The left pedicle screw is in the lateral vertebrae, and no lung injury is seen between the vertebral body and rib. The screw position was not adjusted intraoperatively because it is within the acceptable range.
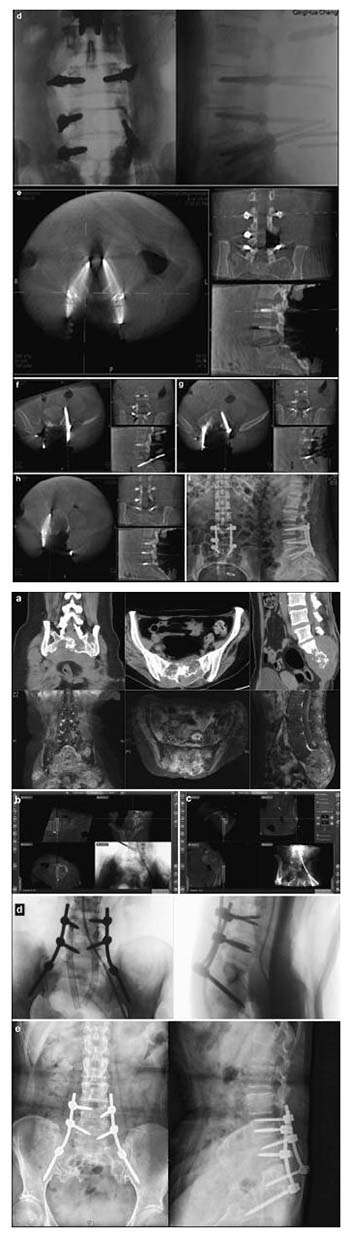
20171023161341 Figure 3 Preoperative, intraoperative, and postoperative images of the lumbar spinal canal of a patient in the internal and external schwannoma resection and pedicle screw fixation group. (a) Lumbar computed tomography (CT) shows an L4-5 intraspinal isodense tumor and a damaged L4 left pedicle and vertebral body. Magnetic resonance imaging (MRI) shows an iso- and hyperintensive signal tumor at L4-5 on the intraspinal T2 image. It is located on the left side of the spinal canal and has invaded a vertebral body and the intervertebral foramen. (b) Fusion of the CT and MRI images, in combination with an intraoperative O-arm and navigation technique, identifies the tumor site and border. (c) Intraoperative L5 pedicle screw implantation is performed under navigation. The screw’s direction, angle, and depth can be seen to match the navigation plan. (d) After screw implantation, an intraoperative O-arm two-dimensional lateral scan shows that the screw position is good. (e) An O-arm three-dimensional (3D) scan shows that the L3 pedicle screw position is good, and does not penetrate the bone cortex. (f) An O-arm 3D scan shows that the L5 left pedicle screw position moves away from the vertebral body and penetrates the rough pedicle bone cortex; (g) An O-arm scan was conducted again to introduce the navigation system as part of the correction of the L5 left pedicle screw, getting it to a good position. (h) An O-arm 3D scan shows that the L4 right pedicle screw position is good. It does not penetrate the bone cortex. Screws are difficult to implant in the left pedicle and vertebral body due to tumor invasion. (i) A lateral lumbar radiography scan, 7 days postoperatively, shows firm screw fixation and good positioning.
20171023161407 Figure 4 Preoperative, intraoperative, and postoperative images of patients in the nearly total sacrococcygeal chordoma resection and pedicle screw fixation group. (a) Lumbosacral vertebral computed tomography shows an S1-3 intraspinal isodense tumor and a severely damaged vertebral body. An enhanced magnetic resonance imaging scan shows S1-3 intraspinal internal and external tumors and a vertebral body that has been invaded and damaged. (b) Intraoperative L4 left pedicle screw implantation is performed under navigation. The direction, angle, and depth of the screw entery can be seen to match the navigation plan. (c) Intraoperative right iliac screw implantation is conducted under navigation. The direction, angle, and depth of the screw entering can be seen according to the navigation plan. (d) After screw implantation, an O-arm two-dimensional lateral scan shows good screw positioning. (e) A lateral lumbar radiographic scan, 7 days postoperatively, shows firm pedicle and iliac screw fixation and good positioning.
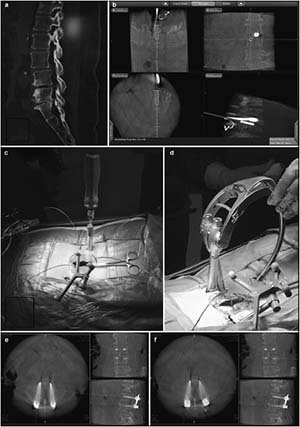
20171023161447 Figure 5 Preoperative, intraoperative, and postoperative images of patients in the percutaneous minimally invasive pedicle internal fixation group. (a) Lumbosacral vertebral computed tomography shows L3 vertebral spondylolisthesis, L3-4 and L4-5 spinal stenosis, intervertebral disc degeneration, and corresponding intervertebral space narrowing. (b) Intraoperative L4 right pedicle screw implantation is performed under navigation. The direction, angle, and depth of screw entry can be seen in real-time, according to the navigation plan. (c, d) Intraoperative screw implantation and bar threading are performed under navigation. (e, f) After screw implantation, O-arm three-dimensional anteroposterior and lateral scans show that the screw is well positioned.
[1]
Odgers IV CJ, Vaccaro AR, Pollack ME, Cotler JM. Accuracy of pedicle screw placement with the assistance of lateral plain radiography. J Spinal Disord 1996, 9(4):334-338.
[2]
Roberts DW, Strohbehn JW, Hatch JF, Murray W, Kettenberger H. A frameless stereotaxic integration of computerized tomographic imaging and the operating microscope. J Neurosurg 1986, 65(4):545-549.
[3]
Steinmann JC, Herkowitz HN, El-Kommos H, Wesolowski DP. Spinal pedicle fixation. Confirmation of an image-based technique for screw placement. Spine 1993, 18(13):1856-1861.
[4]
Cong Y, Bao NR, Zhao JN, Mao GP. Comparing accuracy of cervical pedicle screw placement between a guidance system and manual manipulation:a cadaver study. Med Sci Monit 2015, 21:2672-2677.
[5]
Yang YL, Wang F, Han SM, Wang YH, Dong JL, Li LX, Zhou DS. Isocentric C-arm three-dimensional navigation versus conventional C-arm assisted C1-C2 transarticular screw fixation for atlantoaxial instability. Arch Orthop Trauma Surg 2015, 135(8):1083-1092.
[6]
Tao X, Tian W, Liu B, Li Q, Zhang G. Accuracy and complications of posterior C2 screw fixation using intraoperative three-dimensional fluoroscopy-based navigation. Chin Med J 2014, 127(14):2654-2658.
[7]
Laine T, Lund T, Ylikoski M, Lohikoski J, Schlenzka D. Accuracy of pedicle screw insertion with and without computer assistance:a randomized controlled clinical study in 100 consecutive patients. Eur Spine J 2000, 9(3):235-240.
[8]
Amiot LP, Lang K, Putzier M, Zippel H, Labelle H. Comparative results between conventional and computerassisted pedicle screw insertion in the thoracic, lumbar, and sacral spine. Spine (Phila Pa 1976), 2000, 25(5):606-614.
Oertel MF, Hobart J, Stein M, Schreiber V, Scharbrodt W. Clinical and methodological precision of spinal navigation assisted by 3D intraoperative O-arm radiographic imaging. J Neurosurg Spine 2011, 14(4):532-536.
[11]
Baaj AA, Beckman J, Smith DA. O-arm-based image guidance in minimally invasive spine surgery:technical note. Clin Neurol Neurosurg 2013, 115(3):342-345.
Lange J, Karellas A, Street J, Eck JC, Lapinsky A, Connolly PJ, Dipaola CP. Estimating the effective radiation dose imparted to patients by intraoperative cone-beam computed tomography in thoracolumbar spinal surgery. Spine 2013, 38(5):E306-E312.
[14]
Zhang J, Weir V, Fajardo L, Lin J, Hsiung H, Ritenour ER. Dosimetric characterization of a cone-beam O-arm Imaging system. J Xray Sci Technol 2009, 17(4):305-317.
 2017, Vol. 3
2017, Vol. 3