1 Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing 100050, China;
2 Department of Neural Reconstruction, Beijing Neurosurgery Institute, Capital Medical University, Beijing 100050, China
Gangliocytoma combined with a pituitary adenoma: Reports of three cases and literature review
1 Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing 100050, China;
2 Department of Neural Reconstruction, Beijing Neurosurgery Institute, Capital Medical University, Beijing 100050, China
摘要 Objectives: Sellar gangliocytomas are extremely rare. Since they present clinically and radiologically as pituitary adenomas, the preoperative diagnosis of these mixed tumors is very difficult. Here, we report three cases of gangliocytoma combined with pituitary adenoma and describe our findings. Methods: The clinical data of the three cases of gangliocytoma combined with pituitary adenoma have been retrospectively analyzed, and the published literature has also been reviewed. Results: All three patients underwent pure endonasal endoscopic surgery, and no recurrence was observed over a follow-up of at least 30 months. Growth hormone (GH)-hypersecreting adenoma and tumor calcification were detected in these mixed tumors. Conclusions: Pure endoscopic transnasal transsphenoidal surgery may be an effective way for the treatment of this kind of tumor. Gross total resection of the tumor is recommended. In addition, calcification with GH-hypersecretion may serve as a preoperative diagnostic clue for gangliocytoma in the sella turcica.
Abstract: Objectives: Sellar gangliocytomas are extremely rare. Since they present clinically and radiologically as pituitary adenomas, the preoperative diagnosis of these mixed tumors is very difficult. Here, we report three cases of gangliocytoma combined with pituitary adenoma and describe our findings. Methods: The clinical data of the three cases of gangliocytoma combined with pituitary adenoma have been retrospectively analyzed, and the published literature has also been reviewed. Results: All three patients underwent pure endonasal endoscopic surgery, and no recurrence was observed over a follow-up of at least 30 months. Growth hormone (GH)-hypersecreting adenoma and tumor calcification were detected in these mixed tumors. Conclusions: Pure endoscopic transnasal transsphenoidal surgery may be an effective way for the treatment of this kind of tumor. Gross total resection of the tumor is recommended. In addition, calcification with GH-hypersecretion may serve as a preoperative diagnostic clue for gangliocytoma in the sella turcica.
Zhenmin Wang, Peng Li, Qiangyi Zhou, Zhijun Yang, Pinan Liu. Gangliocytoma combined with a pituitary adenoma: Reports of three cases and literature review[J]. 临床转化神经科学, 2016, 2(3): 165-171.
Zhenmin Wang, Peng Li, Qiangyi Zhou, Zhijun Yang, Pinan Liu. Gangliocytoma combined with a pituitary adenoma: Reports of three cases and literature review. Translational Neuroscience and Clinics, 2016, 2(3): 165-171.
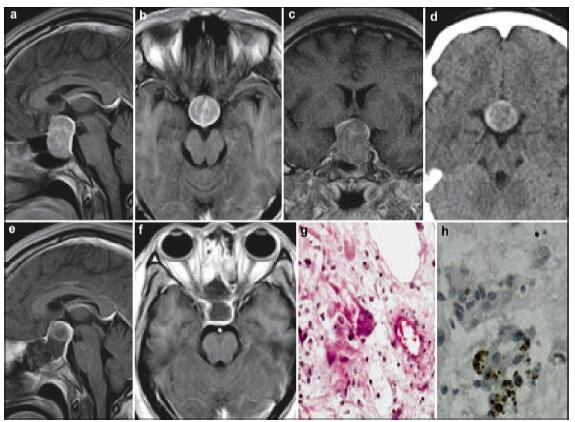
20161117195508 Figure 1 Case 1. The preoperative MRI (a-c) demonstrates an enlarged sella turcica containing an intrasellar mass with a suprasellar extension, showing high density on the CT scan (d). The postoperative MRI shows that the mass lesion was totally removed (e, f). Photomicrographs showing large, sometimes pyramid-shaped cells that are often multinucleated and undergoing atypical mitosis (g, HE, ×200), and positive expression of NSE (h, IHC, ×400). MRI: magnetic resonance imaging; CT: computed tomography; NSE: neuron specific enolase; IHC: immunohistochemistry
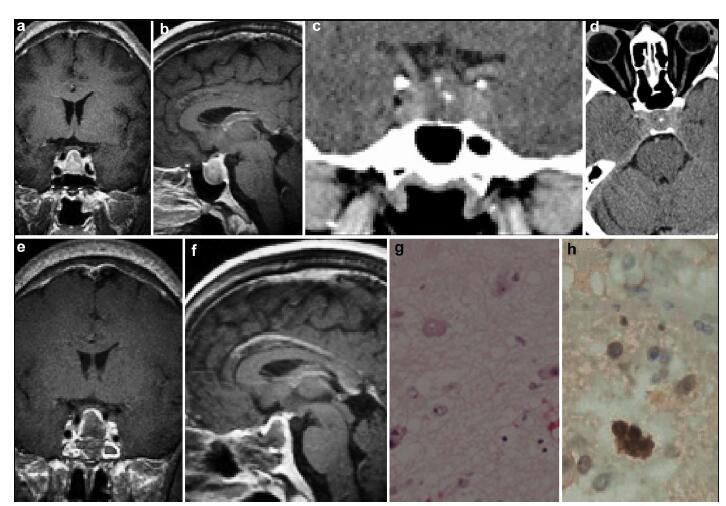
20161117195633 Table 1 The endocrine test results of the three cases
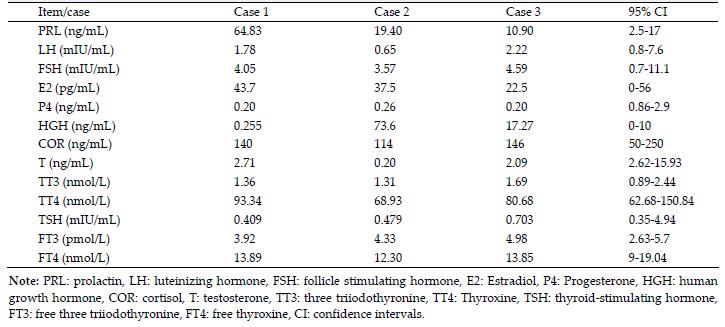
20161117195835 Figure 2 Case 2. The preoperative CT scan (a–c) and MRI (d–f) demonstrate an enlarged sella turcica containing an intrasellar calcified mass with a suprasellar extension, which was totally removed by surgery. Histopathological examination showing multinucleated tumor cells (g, HE, ×200) and NSE positive expression (h, IHC, ×400). MRI: magnetic resonance imaging; CT: computed tomography; NSE: neuron specific enolase; IHC: immunohistochemistry; HE: hematoxylin and eosin.
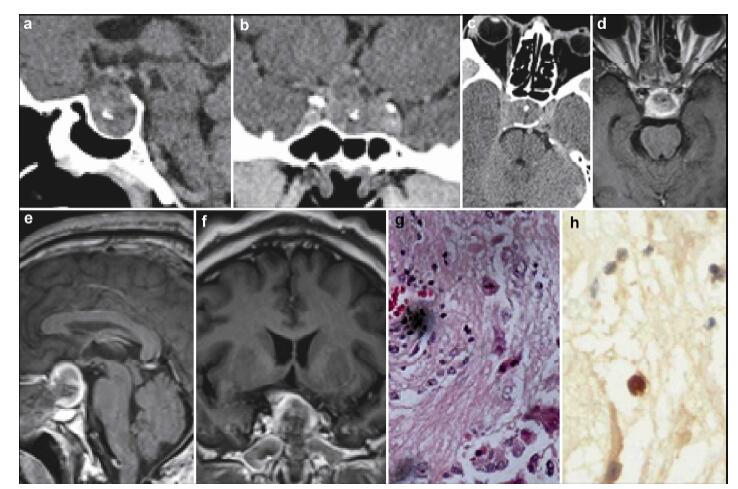
20161117195922 Figure 3 Case 3. A sellar lesion with calcification is observed in the preoperative MRI and CT (a–d), and postoperative MRI (e–f) shows that the lesion has been removed totally. Histopathological examination showing multinucleated tumor cells (g, HE, ×200) , NSE positive expression (h, IHC, ×400). MRI: magnetic resonance imaging; CT: computed tomography; NSE: neuron specific enolase; IHC: immunohistochemistry; HE: hematoxylin and eosin.
[1] Greenfield JG. The pathological examination of forty intracranial neoplasms. Brain 1919, 42(1):29-85.
[2] Geddes JF, Jansen GH, Robinson SF, Gömöri E, Holton JL, Monson JP, Besser GM, Révész T. ‘Gangliocytomas’ of the pituitary:A heterogeneous group of lesions with differing histogenesis. Am J Surg Pathol 2000, 24(4):607-613.
[3] Towfighi J, Salam MM, McLendon RE, Powers S, Page RB. Ganglion cell-containing tumors of the pituitary gland. Arch Pathol Lab Med 1996, 120(4):369-377.
[4] Morikawa M, Tamaki N, Kokunai T, Imai Y. Intrasellar pituitary gangliocyto-adenoma presenting with acromegaly:Case report. Neurosurgery 1997, 40(3):611-614.
[5] Asada H, Otani M, Furuhata S, Inoue H, Toya S, Ogawa Y. Mixed pituitary adenoma and gangliocytoma associated with a cromegaly-Case report. Neurol Med Chir (Tokyo) 1990, 30(8):628-632.
[6] Koutourousiou M, Kontogeorgos G, Wesseling P, Grotenhuis AJ, Seretis A. Collision sellar lesions:Experience with eight cases and review of the literature. Pituitary 2010, 13(1):8-17.
[7] Kurosaki M, Saeger W, Lüdecke DK. Intrasellar gangliocy-tomas associated with acromegaly. Brain Tumor Pathol 2002, 19(2):63-67.
[8] Kontogeorgos G, Mourouti G, Kyrodimou E, Liapi-Avgeri G, Parasi E. Ganglion cell containing pituitary adenomas:Signs of neuronal differentiation in adenoma cells. Acta Neuropathol 2006, 112(1):21-28.
[9] Harding BCA. Malformations. In:Greenfield's Neuro-pathology, 6th ed. Graham DI, Landos PL, Eds. New York:Oxford University Press, 1997.
[10] Asa SL, Scheithauer BW, Bilbao JM, Horvath E, Ryan N, Kovacs K, Randall RV, Laws ER Jr, Singer W, Linfoot JA, Thorner MO, Vale W. A case for hypothalamic acromegaly:A clinicopathological study of six patients with hypothalamic gangliocytomas producing growth hormone-releasing factor. J Clin Endocrinol Metab 1984, 58(5):796-803.
[11] Sano T, Asa SL, Kovacs K. Growth hormone-releasing hormone-producing tumors:Clinical, biochemical, and mor-phological manifestations. Endocr Rev 1988, 9(3):357-373.
[12] Horvath E, Kovacs K, Scheithauer BW, Lloyd RV, Smyth HS. Pituitary adenoma with neuronal choristoma (PANCH):Composite lesion or lineage infidelity? Ultrastruct Pathol 1994, 18(6):565-574.
[13] Vidal S, Horvath E, Kovacs K, Lloyd RV, Smyth HS. Reversible transdifferentiation:Interconversion of somato-trophs and lactotrophs in pituitary hyperplasia. Mod Pathol 2001, 14(1):20-28.
[14] Scheithauer BW, Horvath E, Kovacs K, Lloyd RV, Stefaneanu L, Buchfelder M, Fahlbusch R, von Werder K, Lyons DF. Prolactin-producing pituitary adenoma and carcinoma with neuronal components-A metaplastic lesion. Pituitary 1999, 1(3-4):197-205.
[15] Missale C, Boroni F, Sigala S, Buriani A, Fabris M, Leon A, Dal Toso R, Spano P. Nerve growth factor in the anterior pituitary:Localization in mammotroph cells and cosecretion with prolactin by a dopamine-regulated mechanism. Proc Natl Acad Sci USA 1996, 93(9):4240-4245.
[16] Chen JH, Hersmus N, van Duppen V, Caesens P, Denef C, Vankelecom H. The adult pituitary contains a cell population displaying stem/progenitor cell and early embryonic characteristics. Endocrinology 2005, 146(9):3985-3998.
[17] Garrido E, Becker LF, Hoffman HJ, Hendrick EB, Humphreys R. Gangliogliomas in children. Pediatr Neurosurg 1978, 4(6):339-346.
[18] Takahashi H, Wakabayashi K, Kawai K, Ikuta F, Tanaka R, Takeda N, Washiyama K. Neuroendocrine markers in central nervous system neuronal tumors (gangliocytoma and ganglioglioma). Acta Neuropathol 1989, 77(3):237-243.
[19] Guo YK, Yang ZG, Li Y, Deng YP, Ma ES, Min PQ, Zhang XC. Uncommon adrenal masses:CT and MRI features with histopathologic correlation. Eur J Radiol 2007, 62(3):359-370.
[20] Rha SE, Byun JY, Jung SE, Chun HJ, Lee HG, Lee JM. Neurogenic tumors in the abdomen:Tumor types and imaging characteristics. Radiographics 2003, 23(1):29-43.
[21] Otal P, Mezghani S, Hassissene S, Maleux G, Colombier D, Rousseau H, Joffre F. Imaging of retroperitoneal ganglioneuroma. Eur Radiol 2001, 11(6):940-945.
[22] Van Dyck P, Op de Beeck B, Parizel PM. Helical CT and dynamic MR features of an adrenal ganglioneuroma. JBR-BTR 2006, 89(2):77-79.
[23] Dubois C, Jankowski A, Gay-Jeune C, Chabre O, Pasquier D, Ferretti G. Imaging of adrenal ganglioneuroma:A case report. J Radiol 2005, 86:659-662.
[24] Lonergan GJ, Schwab CM, Suarez ES, Carlson CL. From the archives of the AFIP:Neuroblastoma, ganglioneuroblastoma, and ganglioneuroma:Radiologic-pathologic correlation1. Radiographics 2002, 22(4):911-934.
[25] Scheithauer BW, Kovacs K, Randall RV, Horvath E, Okazaki H, Laws ER Jr. Hypothalamic neuronal hamartoma and adenohypophyseal neuronal choristoma:Their association with growth hormone adenoma of the pituitary gland. J Neuropathol Exp Neurol 1983, 42(6):648-663.
 2016, Vol. 2
2016, Vol. 2