1 Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing 100050, China;
2 Department of Neural Reconstruction, Beijing Neurosurgery Institute, Capital Medical University, Beijing 100050, China
Complete resection of cavernous malformations in the hypothalamus: A case report and review of the literature
1 Department of Neurosurgery, Beijing Tiantan Hospital, Capital Medical University, Beijing 100050, China;
2 Department of Neural Reconstruction, Beijing Neurosurgery Institute, Capital Medical University, Beijing 100050, China
摘要 Objective: Cavernous malformation (CM) originating from the hypothalamus is extremely rare and the deep location presents a challenge for its neurosurgical management. We report such a case to better understand its clinical features. Methods and Results: A 40-year-old male patient presented with impaired vision in the left eye. Magnetic resonance imaging (MRI) revealed a regularly shaped round lesion located in the suprasellar cistern, and a clinical diagnosis of hypothalamic CM was made. Complete microsurgical excision was performed via a right pterional craniotomy. The patient showed good recovery with no further visual acuity or field deficits postoperatively. No CM recurrence or rebleeding was seen on follow-up MRI scans performed over the course of two years. Conclusions: For patients with cavernous malformation in the hypothalamus, accurate preoperative diagnosis with complete surgical removal by an appropriate surgical approach can contribute to satisfactory outcomes.
Abstract: Objective: Cavernous malformation (CM) originating from the hypothalamus is extremely rare and the deep location presents a challenge for its neurosurgical management. We report such a case to better understand its clinical features. Methods and Results: A 40-year-old male patient presented with impaired vision in the left eye. Magnetic resonance imaging (MRI) revealed a regularly shaped round lesion located in the suprasellar cistern, and a clinical diagnosis of hypothalamic CM was made. Complete microsurgical excision was performed via a right pterional craniotomy. The patient showed good recovery with no further visual acuity or field deficits postoperatively. No CM recurrence or rebleeding was seen on follow-up MRI scans performed over the course of two years. Conclusions: For patients with cavernous malformation in the hypothalamus, accurate preoperative diagnosis with complete surgical removal by an appropriate surgical approach can contribute to satisfactory outcomes.
Xingchao Wang, Zhenmin Wang, Zhixian Gao, Pinan Liu. Complete resection of cavernous malformations in the hypothalamus: A case report and review of the literature[J]. 临床转化神经科学, 2016, 2(3): 199-202.
Xingchao Wang, Zhenmin Wang, Zhixian Gao, Pinan Liu. Complete resection of cavernous malformations in the hypothalamus: A case report and review of the literature. Translational Neuroscience and Clinics, 2016, 2(3): 199-202.
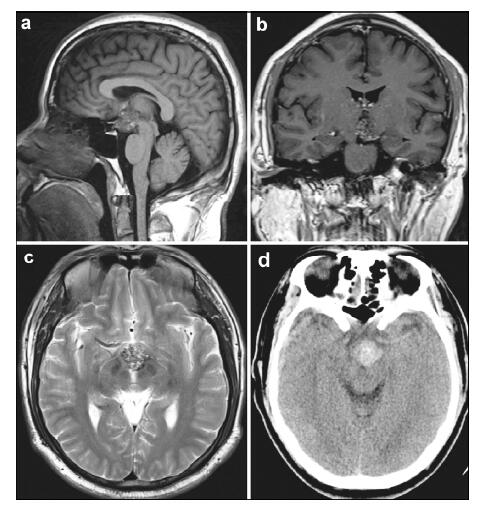
20161117201550 Figure 1 Magnetic resonance imaging (MRI) and computed tomography (CT) of the presurgical hypothalamic cavernous malformation. (a) Sagittal section of T1-weighted MRI shows mixed-signal, round lesions located in the suprasellar cistern. (b) Coronal section of gadolinium-enhanced T1 images show a heterogeneous mild enhancement of the lesion located in hypothalamus. (c) Axial section of T2-weighted MRI shows the lesion’s upward extension into the third ventricle. There was no typical hypointense signal rim around the lesion. (d) Unenhanced computed tomographic imaging reveals a hyperdense lesion in the suprasellar region.
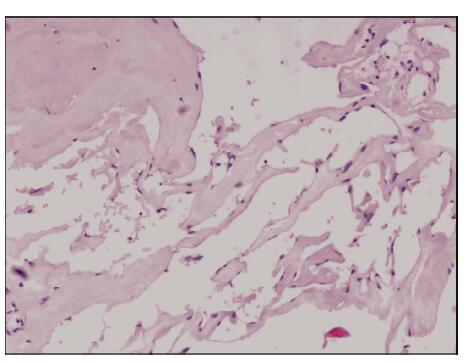
20161117201607 Figure 2 Photomicrograph shows thin-walled cavernous vascular spaces with little intervening brain tissue (Hematoxylin-eosin stain, ×100).
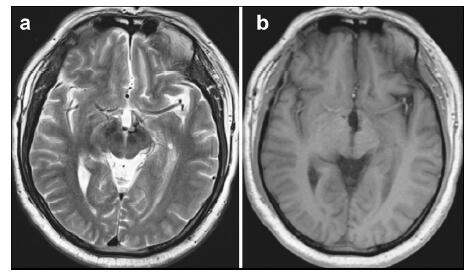
20161117201643 Figure 3 Magnetic resonance imaging (MRI) of the postsurgical hypothalamic cavernous malformation at two-year follow-up. Axial section of T2-weighted (a) and gadolinium-enhanced T1-weighted (b) MRI reveals the complete removal of the hypothalamic cavernous malformation and no evidence of recurrence or rebleeding.
[1]
Batra S, Lin D, Recinos PF, Zhang J, Rigamonti D. Cavernous malformations:Natural history, diagnosis and treatment. Nat Rev Neurol 2009, 5(12):659-670.<br />
[2]
Hassler W, Zentner J, Wilhelm H. Cavernous angiomas of the anterior visual pathways. J Clin Neuroophthalmol 1989, 9(3):160-164.<br />
[3]
Mizutani T, Goldberg HI, Kerson LA, Murtagh F. Cavernous hemangioma in the diencephalon. Arch Neurol 1981, 38(6):379-382.<br />
[4]
Reyns N, Assaker R, Louis E, Lejeune JP. Intraventricular cavernomas:Three cases and review of the literature. Neurosurgery 1999, 44(3):648-654.<br />
[5]
Samii M, Eghbal R, Carvalho GA, Matthies C. Surgical management of brainstem cavernomas. J Neurosurg 2001, 95(5):825-832.<br />
[6]
Abou-Al-Shaar H, Bahatheq A, Takroni R, Al-Thubaiti I. Optic chiasmal cavernous angioma:A rare suprasellar vascular malformation. Surg Neurol Int 2016, 7(Suppl 18):S523-S526.<br />
[7]
Liu JK, Lu Y, Raslan AM, Gultekin SH, Delashaw JB Jr. Cavernous malformations of the optic pathway and hy-pothalamus:Analysis of 65 cases in the literature. Neurosurg Focus 2010, 29(3):E17.<br />
[8]
Mizoi K, Yoshimoto T, Suzuki J. Clinical analysis of ten cases with surgically treated brain stem cavernous angiomas. Tohoku J Exp Med 1992, 166(2):259-267.<br />
[9]
Kurokawa Y, Abiko S, Ikeda N, Ideguchi M, Okamura T. Surgical strategy for cavernous angioma in hypothalamus. J Clin Neurosci 2001, 8 Suppl1:106-108.<br />
[10]
Katayama Y, Tsubokawa T, Maeda T, Yamamoto T. Surgical management of cavernous malformations of the third ventricle. J Neurosurg 1994, 80(1):64-72.<br />
[11]
Rheinboldt M, Blase J. Exophytic hypothalamic cavernous malformation mimicking an extra-axial suprasellar mass. Emerg Radiol 2011, 18(4):363-367.<br />
[12]
Gross BA, Du R. Cerebral cavernous malformations:Natural history and clinical management. Expert Rev Neurother 2015, 15(7):771-777.<br />
[13]
Simard JM, Garcia-Bengochea F, Ballinger WE Jr, Mickle JP, Quisling RG. Cavernous angioma:A review of 126 collected and 12 new clinical cases. Neurosurgery 1986, 18(2):162-172.<br />
[14]
Hempelmann RG, Mater E, Schröder F, Schön R. Complete resection of a cavernous haemangioma of the optic nerve, the chiasm, and the optic tract. Acta Neurochir (Wien) 2007, 149(7):699-703; discussion 703.<br />
[15]
Wang CH, Lin SM, Chen Y, Tseng SH. Multiple deep-seated cavernomas in the third ventricle, hypothalamus and thalamus. Acta Neurochir (Wien) 2003, 145(6):505-508.<br />
[16]
Ogawa Y, Tominaga T. Sellar and parasellar tumor removal without discontinuing antithrombotic therapy. J Neurosurg 2015, 123(3):794-798.<br />
[17]
Hasegawa H, Bitoh S, Koshino K, Obashi J, Kobayashi Y, Kobayashi M, Wakasugi C. Mixed cavernous angioma and glioma (angioglioma) in the hypothalamus-Case report. Neurol Med Chir (Tokyo) 1995, 35(4):238-242.<br />
[18]
Robinson JR, Awad IA, Little JR. Natural history of the cavernous angioma. J Neurosurg 1991, 75(5):709-714.<br />
[19]
Porter RW, Detwiler PW, Spetzler RF, Lawton MT, Baskin JJ, Derksen PT, Zabramski JM. Cavernous malformations of the brainstem:Experience with 100 patients. J Neurosurg 1999, 90(1):50-58.<br />
[20]
Lehner M, Fellner FA, Wurm G. Cavernous haemangiomas of the anterior visual pathways. Short review on occasion of an exceptional case. Acta Neurochir (Wien) 2006, 148(5):571-578.
 2016, Vol. 2
2016, Vol. 2