1 Department of Neurosurgery, Seoul St. Mary's Hospital, College of Medicine, the Catholic University of Korea, Seoul 06591, Republic of Korea;
2 Catholic Neuroscience Institute, College of Medicine, the Catholic University of Korea, Seoul 06591, Republic of Korea;
3 Department of Neurosurgery, Chosun University Hospital, College of Gwangju 61452, Republic of Korea;
4 Department of Neurosurgery, Nowon Eulji Hospital, College of Medicine, Eulji University, Seongnam 826802, Republic of Korea
Long-term results of a simultaneous trial of deep brain and motor cortex stimulation in refractory neuropathic pain
1 Department of Neurosurgery, Seoul St. Mary's Hospital, College of Medicine, the Catholic University of Korea, Seoul 06591, Republic of Korea;
2 Catholic Neuroscience Institute, College of Medicine, the Catholic University of Korea, Seoul 06591, Republic of Korea;
3 Department of Neurosurgery, Chosun University Hospital, College of Gwangju 61452, Republic of Korea;
4 Department of Neurosurgery, Nowon Eulji Hospital, College of Medicine, Eulji University, Seongnam 826802, Republic of Korea
摘要 Objective: Although deep brain stimulation (DBS) and motor cortex stimulation (MCS) are effective in patients with refractory neuropathic pain, their application is still empirical; there is no consensus on which technique is better. Methods: To enhance the success rate of trial stimulation of invasive neuromodulation techniques and identify approapriate stimulation targets in individual patients, we performed a simultaneous trial of thalamic ventralis caudalis (Vc) DBS and MCS in 11 patients with chronic neuropathic pain and assessed the results of the trial stimulation and long-term analgesia. Results: Of the 11 patients implanted with both DBS and MCS electrodes, nine (81.8%) had successful trials. Seven of these nine patients (77.8%) responded to MCS, and two (18.2%) responded to Vc DBS. With long-term follow-up (56 ± 27.5 months), the mean numerical rating scale decreased significantly (P < 0.05). The degree of percentage pain relief in the chronic MCS (n = 7) and chronic DBS (n = 2) groups were 34.1% ± 18.2% and 37.5%, respectively, and there was no significant difference (P = 0.807). Five out of the seven MCS patients (71%) and both DBS patients had long-term success with the treatments, defined as >30% pain relief compared with baseline. Conclusions: With simultaneous trial of DBS and MCS, we could enhance the success rate of invasive trials. Considering the initial success rate and the less invasive nature of epidural MCS over DBS, we suggest that MCS may be a better, initial means of treatment in chronic intractable neuropathic pain. Further investigations including other subcortical target-associated medial pain pathways are warranted.
Abstract: Objective: Although deep brain stimulation (DBS) and motor cortex stimulation (MCS) are effective in patients with refractory neuropathic pain, their application is still empirical; there is no consensus on which technique is better. Methods: To enhance the success rate of trial stimulation of invasive neuromodulation techniques and identify approapriate stimulation targets in individual patients, we performed a simultaneous trial of thalamic ventralis caudalis (Vc) DBS and MCS in 11 patients with chronic neuropathic pain and assessed the results of the trial stimulation and long-term analgesia. Results: Of the 11 patients implanted with both DBS and MCS electrodes, nine (81.8%) had successful trials. Seven of these nine patients (77.8%) responded to MCS, and two (18.2%) responded to Vc DBS. With long-term follow-up (56 ± 27.5 months), the mean numerical rating scale decreased significantly (P < 0.05). The degree of percentage pain relief in the chronic MCS (n = 7) and chronic DBS (n = 2) groups were 34.1% ± 18.2% and 37.5%, respectively, and there was no significant difference (P = 0.807). Five out of the seven MCS patients (71%) and both DBS patients had long-term success with the treatments, defined as >30% pain relief compared with baseline. Conclusions: With simultaneous trial of DBS and MCS, we could enhance the success rate of invasive trials. Considering the initial success rate and the less invasive nature of epidural MCS over DBS, we suggest that MCS may be a better, initial means of treatment in chronic intractable neuropathic pain. Further investigations including other subcortical target-associated medial pain pathways are warranted.
Byung-chul Son, Jin-gyu Choi, Sang-woo Ha, Deog-ryeong Kim. Long-term results of a simultaneous trial of deep brain and motor cortex stimulation in refractory neuropathic pain[J]. 临床转化神经科学, 2017, 3(1): 4-15.
Byung-chul Son, Jin-gyu Choi, Sang-woo Ha, Deog-ryeong Kim. Long-term results of a simultaneous trial of deep brain and motor cortex stimulation in refractory neuropathic pain. Translational Neuroscience and Clinics, 2017, 3(1): 4-15.
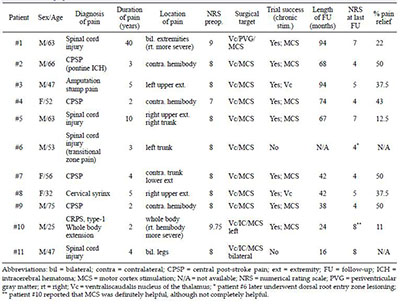
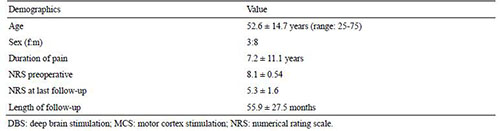
20170512094023 Table 1 Demographics and outcomes of a simultaneous trial of DBS/MCS.
20170512094031 Table 2 Summary of demographics of simultaneous DBS/MCS trial.
20170512094039 Table 3 Long-term results of simultaneous DBS/MCS trial.
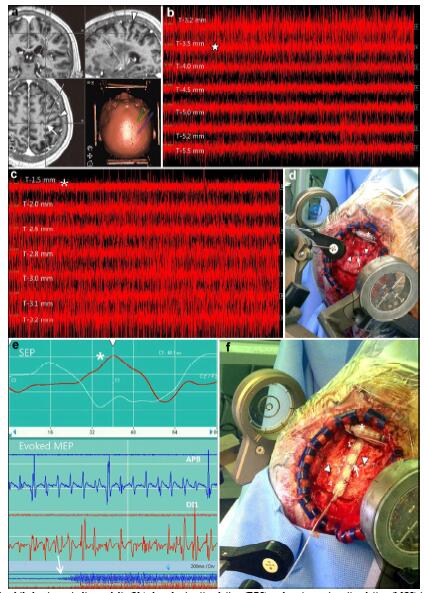
20170512094124 Figure 1 Combined thalamic ventralis caudalis (Vc) deep brain stimulation (DBS) and motor cortex stimulation (MCS) in patient #4. a An image captured from the stereotactic planning software (Framelink®, Medtronic, Minneapolis, MN) during the determination of the initial target coordinates and trajectory planning for the Vc and the hand knob in the precentral gyrus. A white arrow indicates the location of the hand knob corresponding to the hand somatotopy of the precentral gyrus. An arrowhead indicates the central sulcus. b A typical microelectrode recording during exploration of the thalamic Vc nucleus. In the area T-3.5 mm, increased firing of the thalamic sensory nucleus is observed (star), which indicates entrance into the part of the Vc nucleus corresponding to a cutaneous core of the somatotopy. c A microelectrode recording shows an abrupt decrease in the firing of the Vc nucleus (asterisk). This means that the tip of the microelectroderecording probe is located below the thalamic Vc nucleus and is within the white matter. d An intraoperative photograph showing the localization of the precentral gyrus and the central sulcus. An asterisk denotes the implantation of the Vc DBS electrode before MCS. Arrow heads indicate the marking of the course of the central sulcus over the dura mater and an arrow indicates the location of the target for the precentral gyrus. e An image showing the phase reversal (asterisk) of the somatosensory evoked potential (SEP) in the upper image. The lower image shows a motor evoked potential (MEP) response taken from the abductor policis brevis (APB) and the first dorsal interossoeus muscles (DI1) through macrostimulation of the contacts of the paddle lead over the precentral gyrus. An arrow shows the elicitation of the MEP in the contralateral hand muscles. f An intraoperative photograph showing the placement of paddle lead for MCS. The contact “2” of the paddle lead is placed on the target for the precentral gyrus. A dotted line (arrowheads) denotes the course of the central sulcus and an arrow indicate the location of the predetermined MCS target.
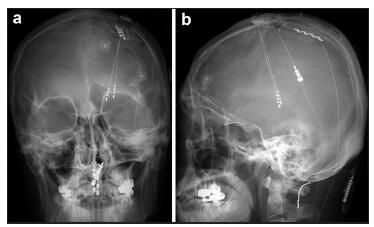
20170512094150 Figure 2 Anterior-posterior a and lateral b projections of skull x-ray films of a patient (#10) who underwent a simultaneous DBS/ MCS trial for intractable, chronic neuropathic pain. This patient had both thalamic Vc and internal capsule DBS electrodes combined with a left-side MCS electrode. Note the previously implanted C1–C2 paddle lead for treatment-resistant complex regional pain syndrome with whole-body involvement, which was more severe in the right hemibody. In this particular patient, we obtained >50% pain relief with the initial MCS trial. However, thalamic Vc stimulation aggravated the hemibody pain. The prominent analgesic effect of MCS faded postoperatively within six months. However, the patient still today (24 months after MCS) uses chronic MCS for unremitting pain. He judged MCS as being much more effective than spinal cord stimulation.
 2017, Vol. 3
2017, Vol. 3