| Original Articles |
|


|
|
|
| Malignant transformation and treatment of cystic mixed germ cell tumor |
| Yapeng Zhao1, Hongyu Duan2, Qinghui Zhang1,2, Bingxin Shi1, Hui Liang2, Yuqi Zhang1,2 |
1 The Medical Center, Tsinghua University, Beijing 100084, China;
2 Department of Neurosurgery, Tsinghua University Yuquan Hospital, Beijing 100040, China |
|
|
|
|
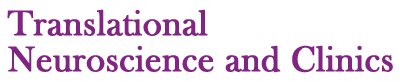
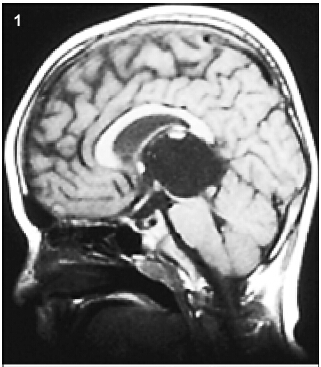
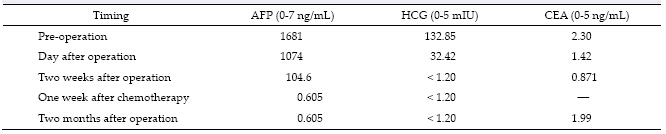
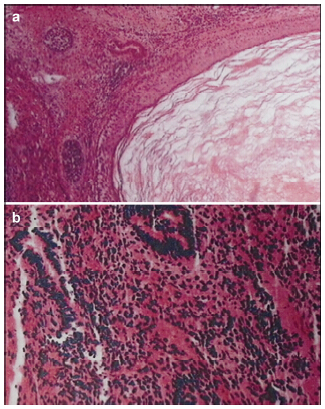
Abstract Objective: The authors report an extremely unusual presentation and management of a children pineal mixed germ cell tumor mainly composed of immature teratoma, aiming to summarize main theraptic points by literature review. Methods: A cystic lesion located in the rear of third ventricle in a child was detected 3 years ago with no other therapy performed except for a ventriculo-peritoneal shunt. During the following 3 years, intermitted regular brain MRI demonstrated no evidence of lesion aggrandizement. However from 20 days before admission to our institute the patient began to present acutely with exacerbating clinical symptoms meanwhile brain MRI showed signs of abrupt revulsions of initial lesion without any incentive cause. Neurological examination revealed a significant rising of serum tumor marker level. Then surgical resection was performed immediately after admission which was followed by correlative two-course chemotherapy. Results: Postoperative brain MRI demonstrated totally removing of the lesion in rear of third ventricle. Serum tumor marker level decreased remarkably after surgery and declined to normal level after two-course chemotherapy. No obvious neurological deficit occurred except for short-term memory difficulty which gradually recovered within two weeks. Soon after the second course chemotherapy the patient was currently asymptomatic and returned to school. Conclusions: (1) To ensure definitive diagnosis and proper therapecutic protocols benefit from grasping clinical features of mixed germ cell tumor. (2) Overall preoperative investigation including serum tumor marker level is as critical as neurological imaging examination. (3) Surgical excision is confirmed to be the key modality of treatment. With the regarding of mixed germ cell tumor, never highlight total resection too much. (4) Postoperative adjuvant chemotherapy is recommended as further intensive treatment to improve the prognosis of mix germ cell tumor.
|
|
Received: 03 December 2015
Published: 31 March 2016
|
|
Corresponding Authors:
Yuqi Zhang, E-mail: yuqi9597@sina.com
E-mail: yuqi9597@sina.com
|
|
|
[1] Canan A, Gülsevin T, Nejat A, Tezer K, Sule Y, Meryem T, Gülsen E. Neonatal intracranial teratoma. Brain Dev 2000, 22(5): 340-342.
[2] Matsutani M, Sano K, Takakura K, Fujimaki T, Nakamura O, Funata N, Seto T. Primary intracranial germ cell tumors: A clinical analysis of 153 histologically verified cases. J Neurosurg 1997, 86(3): 446-455.
[3] Kakani AB, Karmarkar VS, Deopujari CE, Shah RM, Bharucha NE, Muzumdar G. Germinoma of fourth ventricle: A case report and review of literature. J Pediatr Neurosci 2006, 1(1): 33-35.
[4] Jorsal T, Rørth M. Intracranial germ cell tumours. A review with special reference to endocrine manifestations. Acta Oncol 2012, 51(1): 3-9.
[5] O'Grady J, Kobayter L, Kaliaperumal C, O'Sullivan M. ‘Teeth in the brain'—A case of giant intracranial mature cystic teratoma. BMJ Case Rep 2012, pii: bcr0320126130, doi: 10.1136/bcr.03.2012.6130.
[6] Sanyal P, Barui S, Mathur S, Basak U. A case of mature cystic teratoma arising from the fourth ventricle. Case Rep Pathol 2013, 2013: 702424.
[7] Noudel R, Vinchon M, Dhellemmes P, Litré CF, Rousseaux P. Intracranial teratomas in children: The role and timing of surgical removal. J Neurosurg Pediatr 2008, 2(5): 331-338.
[8] Shim KW, Kim DS, Choi JU, Kim SH. Congenital cavernous sinus cystic teratoma. Yonsei Med J 2007, 48(4): 704-710.
[9] Moiyadi A, Jalali R, Kane SV. Intracranial growing teratoma syndrome following radiotherapy—An unusually fulminant course. Acta Neurochir 2010, 152(1): 137-142.
[10] Bi WL, Bannykh SI, Baehring J. The growing teratoma syndrome after subtotal resection of an intracranial nongerminomatous germ cell tumor in an adult: Case report. Neurosurgery 2005, 56(1): 188.
[11] Hanna A, Edan C, Heresbach N, Ben HM, Guegan Y. Expanding mature pineal teratoma syndrome. Case report. Neuro-Chirurgie 2000, 46(6): 568-572.
[12] Yagi K, Kageji T, Nagahiro S, Horiguchi H. Growing teratoma syndrome in a patient with a non-germinomatous germ cell tumor in the neurohypophysis-case report. Neurol Med Chir 2004, 44(1): 33-37.
[13] André F, Fizazi K, Culine S, Droz JP, Taupin P, Lhommé C, Terrier-Lacombe M-J, Théodore, C. The growing teratoma syndrome: Results of therapy and long-term follow-up of 33 patients. Eur J Cancer 2000, 36(11): 1389-1394.
[14] Shim KW, Kim DS, Choi JU. Mixed or metachronous germ-cell tumor? Child's Nerv Syst 2007, 23(6): 713-718.
[15] Jia G, Zhang YQ, Ma ZY, Luo SQ, Dai K. The clinical study on the treatment of the introcranial mature teratoma and immature teratoma: 37 case reports. Chin J Neurosurg 2000, 19(5): 334-336. (in Chinese)
[16] Yamashita N, Kanai H, Kamiya K, Yamada K, Togari H, Nakamura T. Immature teratoma producing alpha-fetoprotein without components of yolk sac tumor in the pineal region. Child's Nerv Syst 1997, 13(4): 225-228.
[17] Sun T, Tian YJ, Liu R, Wan WQ, Luo SQ, Li CD. Clinical features, diagnosis, and treatment of primary intracranial choriocarcinoma in children. Chin J Neurosurg 2015, 31(11): 1094-1098. (in Chinese)
[18] Bruce JN, Stein BM. Surgical management of pineal region tumors. Acta Neurochir 1995, 134(3-4): 130-135.
[19] Friedman JA, Lynch JJ, Buckner JC, Scheithauer BW, Raffel C. Management of malignant pineal germ cell tumors with residual mature teratoma. Neurosurgery 2001, 48(3): 518-523.
[20] Ma ZY, Zhang YQ, Luo SQ. Transcallosal-interfornix approach to remove the tumors of the third ventricle in children. Chin J Neurosurg 2000, 16(4): 207-209. (in Chinese)
[21] Fukuoka K, Yanagisawa T, Suzuki T, Wakiya K, Matsutani M, Sasaki A. Nishikawa R. Successful treatment of hemorrhagic congenital intracranial immature teratoma with neoadjuvant chemotherapy and surgery. J Neurosurg Pediatr 2014, 13(1): 38-41.
[22] Severino M, Schwartz ES, Thurnher MM, Rydland J, Nikas I, Rossi A. Congenital tumors of the central nervous system. Neuroradiology 2010, 52(6): 531-548.
[23] Zhu T, Yu YH, Zhang DJ, Zhang JN, Zhang YQ. Clinical analysis of central nervous system tumors in children, a report of 468 cases. Chin J Neurosurg 2012, 28(1): 8-12. (in Chinese)
[24] Gong J, Jia G, Zhang YQ, Li CD, Tian YJ, Ma ZY. Early diagnosis and comprehensive treatment for germinoma of sellar region. Chin J Minim Invasive Neurosurg 2012, 17(6): 245-247. (in Chinese)
[25] Wang ZD, Jia G, Ma ZY, Zhang YQ, Yao HX. Long-term recurrence after total resection of intracranial mature teratoma: 2 case report and literature review. Chin J Minim Invasive Neurosurg 2009, 14(1): 18-19. (in Chinese)
[26] Li Q, Zhang YQ. Diagnosis and treatment of intracranial germinoma. Chin J Neurosurg 2008, 24(6): 479-480. (in Chinese)
[27] Wu MC, Luo SQ, Jia G, Ma ZY, Zhang YQ. Intracranial nongerminomatous malignant germ cell tumors. Chin J Neurosurg 2006, 22(4): 199-203. (in Chinese) |
|
Viewed |
|
|
|
Full text
|
|
|
|
|
Abstract
|
|
|
|
|
Cited |
|
|
|
|
| |
Shared |
|
|
|
|
| |
Discussed |
|
|
|
|