Resection of intramedullary spinal cord tumor under awake anesthesia: A novel approach to minimize postoperative motor deficits
Ahsan Ali Khan1, Lukui Chen1, Xiaoyuan Guo1, Hong Wang1, Guojian Wu1, Jun Kong1, Ning Yin2
1 Department of Neurosurgery, Zhongda Hospital, Southeast University, Nanjing 210009, China;
2 Department of Anaesthesia, Zhongda Hospital, Southeast University, Nanjing 210009, China
Resection of intramedullary spinal cord tumor under awake anesthesia: A novel approach to minimize postoperative motor deficits
Ahsan Ali Khan1, Lukui Chen1, Xiaoyuan Guo1, Hong Wang1, Guojian Wu1, Jun Kong1, Ning Yin2
1 Department of Neurosurgery, Zhongda Hospital, Southeast University, Nanjing 210009, China;
2 Department of Anaesthesia, Zhongda Hospital, Southeast University, Nanjing 210009, China
摘要 Objective: To observe advantages and disadvantages of the resection of intramedullary spinal cord tumor under awake anesthesia. Methods: Two patients with intramedullary spinal cord tumor underwent resection under awake anesthesia and followed up post-operatibely for any motor deficits. Results: Patients who underwent tumor resection under awake (AAA) anesthesia combined with intraoperative NPM had no motor deficits postoperatively. More accurate and nondelayed responses were observed in the awake cycle of anesthesia and helped guide surgery, thus avoiding injuries to the spinal cord. Conclusion: Intramedullary spinal cord tumors are not common, but only gross total resection (GTR) can provide complete remission of symptoms and progression-free survival. However, GTR sometimes results in motor function deficits postoperatively, particularly when the cervical cord is involved, and especially if surgery is done under general anesthesia with intraoperative neurophysiological monitoring (NPM) alone, because of delayed sensory evoked potential and motor evoked potential responses. We present two cases that underwent GTR of cervical intramedullary spinal cord tumors under an asleep-awake-asleep (AAA) cycle of anesthesia, combined with intraoperative NPM in which no post-operative motor deficits were observed on 6-months hs follow up.
Abstract: Objective: To observe advantages and disadvantages of the resection of intramedullary spinal cord tumor under awake anesthesia. Methods: Two patients with intramedullary spinal cord tumor underwent resection under awake anesthesia and followed up post-operatibely for any motor deficits. Results: Patients who underwent tumor resection under awake (AAA) anesthesia combined with intraoperative NPM had no motor deficits postoperatively. More accurate and nondelayed responses were observed in the awake cycle of anesthesia and helped guide surgery, thus avoiding injuries to the spinal cord. Conclusion: Intramedullary spinal cord tumors are not common, but only gross total resection (GTR) can provide complete remission of symptoms and progression-free survival. However, GTR sometimes results in motor function deficits postoperatively, particularly when the cervical cord is involved, and especially if surgery is done under general anesthesia with intraoperative neurophysiological monitoring (NPM) alone, because of delayed sensory evoked potential and motor evoked potential responses. We present two cases that underwent GTR of cervical intramedullary spinal cord tumors under an asleep-awake-asleep (AAA) cycle of anesthesia, combined with intraoperative NPM in which no post-operative motor deficits were observed on 6-months hs follow up.
Ahsan Ali Khan, Lukui Chen, Xiaoyuan Guo, Hong Wang, Guojian Wu, Jun Kong, Ning Yin. Resection of intramedullary spinal cord tumor under awake anesthesia: A novel approach to minimize postoperative motor deficits[J]. 临床转化神经科学, 2017, 3(1): 28-34.
Ahsan Ali Khan, Lukui Chen, Xiaoyuan Guo, Hong Wang, Guojian Wu, Jun Kong, Ning Yin. Resection of intramedullary spinal cord tumor under awake anesthesia: A novel approach to minimize postoperative motor deficits. Translational Neuroscience and Clinics, 2017, 3(1): 28-34.
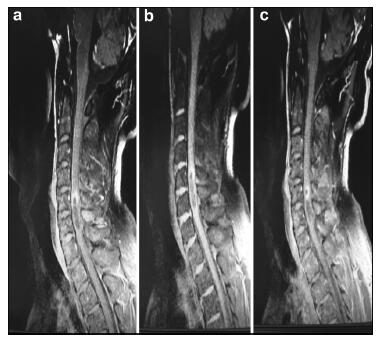
20170512093634 Figure 1 a–c. Preoperative MR images of Case 1.
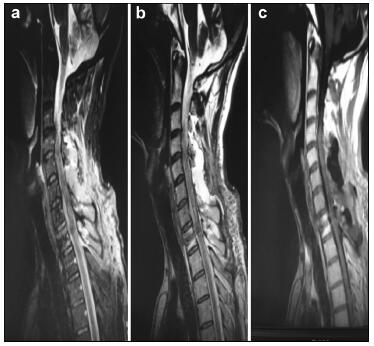
20170512093647 Figure 2 a–c. Postoperative MR images of Case 1.
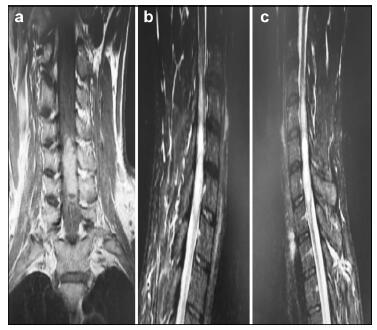
20170512093703 Figure 3 a–c. Preoperative MR images of Case 2.
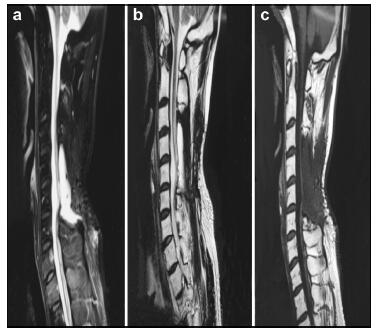
20170512093715 Figure 4 a–c. Postoperative MR images of Case 2.
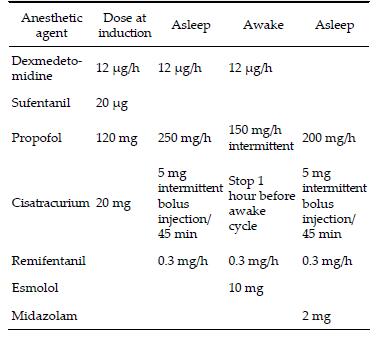
20170512093728 Table 1 Pharmacological agents used for anesthesia induction and AAA cycle.
[1]
Klekamp J, Samii M. Surgery of Spinal Tumors. Berlin Heidelberg: Springer, 2007.
[2]
McCormick PC, Stein BM. Intramedullary tumors in adults. Neurosurg Clin N Am 1990, 1(3): 609-630.
[3]
Wang ZY, Sun JJ, Xie JC, Li ZD, Ma CC, Liu B, Chen XD, Liao HI, Yu T, Zhang J. Comparative analysis on the diagnosis and treatments of multisegment intramedullary spinal cord tumors between the different age groups. Neurosurg Rev 2012, 35(1): 85-93.
[4]
Kim SH, Bak KH, Kim DW, Kang TH. Primary intramedullary spinal sarcoma: A case report and review of the current literatures. J Korean Neurosurg Soc 2010, 48(5): 448-451.
[5]
McGirt MJ, Goldstein IM, Chaichana KL, Tobias ME, Kothbauer KF, Jallo GI. Extent of surgical resection of malignant astrocytomas of the spinal cord: Outcome analysis of 35 patients. Neurosurgery 2008, 63(1): 55-61.
[6]
Beneš VIII, Barsa P, Beneš VJr, Suchomel P. Prognostic factors in intramedullary astrocytomas: A literature review. Eur Spine J 2009, 18(10): 1397-1422.
[7]
Garcés-Ambrossi GL, McGirt MJ, Mehta VA,Sciubba DM, Witham TF, Bydon A, Wolinksy JP, Jallo GI, Gokaslan ZL. Factors associated with progression-free survival and longterm neurological outcome after resection of intramedullary spinal cord tumors: Analysis of 101 consecutive cases. J Neurosurg Spine 2009,11(5): 591-599.
[8]
Chi JH, Parsa AT. Intramedullary spinal cord metastasis: Clinical management and surgical considerations. Neurosurg Clin N Am 2006, 17(1): 45-50.
[9]
Abdel-Wahab M, Etuk B, Palermo J, Shirato H, Kresl J, Yapicier O, Walker G, Scheithauer BW, Shaw E, Lee C, et al. Spinal cord gliomas: A multi-institutional retrospective analysis. Int J Radiat Oncol Biol Phys 2006, 64(4): 1060-1071.
[10]
Blanshard HJ, Chung F, Manninen PH, Taylor MD, Bernstein M. Awake craniotomy for removal of intracranial tumor: Considerations for early discharge. Anesth Analg 2001, 92(1): 89-94.
[11]
Pereira LCM, Oliveira KM, L'Abbate GL, Sugai R, Ferreira JA, da Motta LA. Outcome of fully awake craniotomy for lesions near the eloquent cortex: Analysis of a prospective surgical series of 79 supratentorial primary brain tumors with long follow-up. Acta Neurochir(Wien) 2009, 151(10): 1215-1230.
[12]
De Benedictis A, Moritz-Gasser S, Duffau H. Awake mapping optimizes the extent of resection for low-grade gliomas in eloquent areas. Neurosurgery 2010, 66(6): 1074-1084.
[13]
Chacko AG, Thomas SG, Babu KS, Daniel RT, Chacko G, Prabhu K, Cherian V, Korula G. Awake craniotomy and electrophysiological mapping for eloquent area tumours. Clin Neurol Neurosurg 2013, 115(3): 329-334.
[14]
de Amorim RLO, de Almeida AN, de Aguiar PHP, Fonoff ET, Itshak S, Fuentes D, Teixeira MJ. Cortical stimulation of language fields under local anesthesia: Optimizing removal of brain lesions adjacent to speech areas. Arq Neuropsiquiatr 2008, 66(3A): 534-538.
[15]
Hoshimaru M, Koyama T, Hashimoto N, Kikuchi H. Results of microsurgical treatment for intramedullary spinal cord ependymomas: Analysis of 36 cases. Neurosurgery 1999, 44(2): 264-269.
[16]
Jallo GI, Freed D, Epstein F. Intramedullary spinal cord tumors in children. Childs Nerv Syst 2003, 19(9): 641-649.
Morota N, Deletis V, Constantini S, Kofler M, Cohen H, Epstein FJ. The role of motor evoked potentials during surgery for intramedullary spinal cord tumors. Neurosurgery 1997, 41(6): 1327-1336.
[19]
Matsuyama Y, Sakai Y, Katayama Y, Imagama S, Ito Z, Wakao N, Sato K, Kamiya M, Yukawa Y, Kanemura T, et al. Surgical results of intramedullary spinal cord tumor with spinal cord monitoring to guide extent of resection. J Neurosurg Spine 2009, 10(5): 404-413.
[20]
Cristante L, Herrmann HD. Surgical management of intramedullary spinal cord tumors: Functional outcome and sources of morbidity. Neurosurgery 1994, 35(1): 69-76.
[21]
Sandalcioglu IE, Hunold A, Müller O, Bassiouni H, Stolke D, Asgari S. Spinal meningiomas: Critical review of 131 surgically treated patients. Eur Spine J 2008, 17(8): 1035-1041.
Yang SY, Yang XY, Hong GL. Surgical treatment of one hundred seventy-four intramedullary spinal cord tumors. Spine 2009, 34(24): 2705-2710.
[24]
Boström A, Kanther NC, Grote A, Boström J. Management and outcome in adult intramedullary spinal cord tumours: A 20-year single institution experience. BMC Res Notes 2014, 7: 908.
 2017, Vol. 3
2017, Vol. 3